As someone who got #HepC via Vertical transmission, I don’t just have a lot of thoughts on the matter, I tend to make a lot of comments, public ones. The CDC’s new expansion incorporates almost all of the concerns I’ve voiced to the CDC, CDPH and others over the years when they solicit input from the community.
The latest MMWR from the CDC goes into The escalating prevalence of Hepatitis C Virus (HCV) infections, particularly among reproductive-aged and pregnant populations, underscores a burgeoning health challenge. The Centers for Disease Control and Prevention (CDC) revamped its guidelines in 2020 to encompass universal screening for adults and pregnant individuals, aiming to adeptly manage and curb the proliferation of this ailment.
Epidemiological Trends:
The surge in HCV infections since 2010 is alarming, with acute cases notably tripling among individuals aged 20-39. This uptick correlates with an increase in injection drug use, necessitating targeted interventions. The domino effect of escalating acute infections to chronic conditions emphasizes the urgency for early detection and management. (There’s likely to be a systems issue here, based on a lack of accessible mental health management options, and likely increases in self-medication, among a myriad of other co-occurring circumstances and conditions)
Transmission Dynamics:
Percutaneous exposure to infected blood, predominantly through injection drug use, is a significant transmission route. Perinatal transmission is another vector of concern, thus necessitating prudent strategies to mitigate HCV spread from mother to infant. Understanding these transmission dynamics is pivotal for devising effective preventive frameworks. But its important not to judge people, based on data, rather its imperative we support the person through their diagnosis to cure, as it helps reduce stigma and potential resulting trauma.
Testing, Diagnosis and why this change is important:
The CDC’s 2020 guidelines update underscored universal screening to foster early detection and management. The guidelines propose refined testing protocols for infants and children born to HCV-infected mothers, mirroring the advancements in HCV testing methodologies. This was made possible in part due to public comments from fantastic folks like yourself!
Clinical Progression of Perinatally Acquired HCV Infection:
The variance in clinical progression among perinatally infected children underscores the need for timely interventions. While some achieve spontaneous clearance, others advance to chronic infections, necessitating vigilant monitoring and management to avert severe liver disease. (That’s me, they’re talkin’ bout me ya’ll, End Stage Liver Disease by age 22)
The recent CDC guidelines expand on the diagnostic procedures for HCV infection in pregnant individuals and perinatally infected children. The shift from risk-based to universal screening for HCV during pregnancy aims to bridge the previous under-diagnosis gap. A notable uptick in HCV screening during pregnancy has been witnessed, and all professional societies now advocate for testing perinatally exposed infants for HCV, albeit with variations in the timing.
Clinical Management and Treatment of Perinatal HCV Infection highlights a 6%-7% transmission rate of HCV among perinatally exposed children, (this is almost twice as high as when I was diagnosed with HepC in 1999) with Direct-Acting Antiviral (DAA) therapy emerging as a viable treatment avenue for children aged ≥3 years. The CDC, along with other professional bodies like AASLD-IDSA and NASPGHAN, is steering towards maximizing early diagnosis and linkage to care through perinatal testing for HCV.
Great, but What are the CDC’s new testing recommendations for Hepatitis C Testing Among Perinatally Exposed Infants and Children?
Perinatally exposed infants should receive a NAT for HCV RNA at age 2–6 months to identify children in whom chronic HCV infection might develop if not treated. (Importantly it skips the Antibody test, because the test could indicate a false positive, capturing the maternal antibodies, TBH the antibody test, while a useful epidemiological tool, does beg the question as it to its usefulness for children at all, when, at least anecdotally, it causes a lot of confusion for patients.)
-Infants with detectable HCV RNA should be managed in consultation with a health care provider with expertise in pediatric hepatitis C management.
-Infants with an undetectable HCV RNA result do not require further follow-up unless clinically warranted.
-Infants and children aged 7–17 months who are perinatally exposed to HCV and have not previously been tested should receive a NAT for HCV RNA.
-Children aged ≥18 months who are perinatally exposed to HCV and have not previously been tested should receive an anti-HCV test with reflex to NAT for HCV RNA (Figure 4). (This is an interesting update because it helps with follow-up and appropriate diagnosis, it also shores up holes in terms of late diagnosis, like in my case, where my mom was diagnosed when I was 12, albeit because of my positive case. Although if someone has a negative NAT HCV RNA result, it would seem unnecessary to do an antibody test, which again, just reiterating the likely waste of time and resources of an antibody test.)
Figure 4 from CDC MMWR Recommendations and Reports / November 3, 2023
Cost-Effectiveness Considerations, The CDC conducted a novel analysis to evaluate the cost-effectiveness of perinatal Hepatitis C Virus (HCV) testing strategies, comparing the current method of testing at 18 months to a proposed strategy of testing at 2-6 months. The mathematical modeling study revealed that earlier testing yielded increased diagnoses, improved health outcomes, and was cost-saving at a population level, with savings of $469,671 per year. Universal screening strategies, although enhancing diagnoses and health outcomes, were found to be less cost-effective. The study, evaluated for quality via the CHEERS checklist, substantiated that testing known exposed infants at 2-6 months is both cost-effective and beneficial for better health outcomes.
Hepatitis C Elimination
Ongoing monitoring and potentially revising recommendations in line with evolving epidemiology and treatment modalities for hepatitis C during pregnancy and among children are on the CDC’s radar. The quest for more data on universal screening, prevalence rates among pregnant persons, and the natural history of perinatal hepatitis C is unending. The deployment of highly sensitive and specific NATs for RNA detection among perinatally exposed infants and children is a beacon of hope in identifying those with HCV infection. This initiative aligns with the broader agenda of national hepatitis C elimination goals, showcasing a concerted effort to ensure no population is left behind in this health crusade. The road towards hepatitis C elimination is laden with challenges, yet with cohesive strategies and relentless pursuit of early diagnosis and treatment, strides towards a healthier tomorrow are within grasp. As someone who understands the impact of a pediatric diagnosis of Hepatitis C, in terms of the emotional experience, and challenge with family interactions and stigma, this is a welcome update to capture potential cases that might otherwise be missed.
Get Tested, Get Treatment, Let’s End Hep C!
Panagiotakopoulos L, Sandul AL, et al. CDC Recommendations for Hepatitis C Testing Among Perinatally Exposed Infants and Children — United States, 2023. MMWR Recomm Rep 2023;72(No. RR-4):1–19. DOI: http://dx.doi.org/10.15585/mmwr.rr7204a1
Well, this was supposed to be about the economy, but that’ll come later. While each of these *can* be read independently, it’s best when read together: First Article, and Second Article.
First, let’s talk about the title of the article, “Trust me, it’s raining.” We’re diving into the importance of public trust in agencies and how, unfortunately, science isn’t always the driver of a decision as much as we’d like to think it is. Because in May, the C.D.C. and the Biden Administration’s messaging was akin to pissing on our shoes and telling us it was raining. Unfortunately for us, when it rains, it pours.
It’s also meant as an analogy we’ll talk about later when it comes to preparing the tools in your intervention toolbox, how they layer, and how to think about daily covid protection, more like weather, or well, rain.
A few weeks ago, amid the new mask rules, the C.D.C. also acknowledged that transmission has been occurring among the vaccinated population. For some reason, this tidbit seems to be very misleading among folks, from advancing concerns about the effectiveness of the vaccine vs. the new fears of Delta/V.O.C.s… but this reality makes their previous guidance seem suspect.
Because in terms of the data and Literature at the time, it was. It was a political decision to not simply repeal the mask guidance prematurely, but to encourage abandonment of interventions once vaccinated… Public Health experts have been beside themselves this entire time. When vaccination rates scuttled, the hope that F.O.M.O. would encourage folks to get vaccinated not only fell flat but helped encourage cases to spread.
In my previous articles, I’ve explained the reality reservoirs play when large groups of folks refuse to abide by interventions designed to decrease the incidence of COVID19. Those being mask-wearing, physical distancing, increased hygiene/handwashing, and of course vaccination when medically reasonable.
Before we dive into why the new C.D.C. guidance makes sense and how we should incorporate the new “covid weather map” into our daily lives, let’s talk about that last intervention.
The vaccines are solid, they work well,and are unlikely to require a booster any time soon. In November/December, that may change. (although the WHO, taking a political knee and saying please stall until September for boosters to the developed countries pushing boosters)It’s important that the target for vaccination should be the most folks getting fully vaccinated before boosters become common in developed countries, if we want to eliminate the global recurrence of new VOCS at the rapid pace we’ve seen. “In the context of ongoing global vaccine supply constraints, administration of booster doses will exacerbate inequities by driving up demand and consuming scarce supply while priority populations in some countries, or subnational settings, have not yet received a primary vaccination series. The focus for the time being remains on increasing global vaccination coverage with the primary series (either one or two doses for current EUL vaccines).” as stated by the W.H.O.
That being said, if our current V.O.C. trend continues, sometime next year, a booster would likely help the more vulnerable populations and may be indicated for everyone should the virus find new footholds. The science behind boosters is sound, and the data reflects the protective quality of the vaccine. We have always known that the vaccine likely protects to a certain degree against infection but that it does not always prevent transmission.
All my pencils just say Drugs now
Our current messaging on the pandemic is, well… bad. It’s exclusive, shame-inducing, and it’s basically the same strategy we always use: shame, aka peer pressure. Does it work? To a degree, but it has a weak range of effectiveness, it always has; Project D.A.R.E. is ineffective(West, 2004). If you suspect it works, I D.A.R.E. you to consider other similar strategies met with bucking shame and tribalism like the “War on Drugs” and, well, Condom use.
When we hear messaging on vaccination, it blames the unvaxxed for all the problems we’re experiencing, as if they are the source of the new problems. Which while partially accurate regarding V.O.C.s, it’s also important to remember that this is a virus. And no one is at fault here.
Leaders who use their platform to spread misinformation or disincentivize folks from taking the vaccine or following other interventions do bear a degree of blame for which society should interpret sooner rather than later.
It’s important to consider the US CDC messaging isn’t happening in a vacuum, it’s happening in a world where 20-30% of the population cannot afford the vaccine under the current conditions, and somewhere around 20% are struggling to access for a lot of different reasons, but mostly to do with cost or the convenient opportunity to commit genocide with less potential blame. Currently, about 30.4% of the world is at least partially vaccinated, only 15.8 are fully vaccinated, and the U.S. just passed the 50% mark on fully vaccinated (two weeks after the last jab.) Pandemic is global, an important reminder here is that V.O.C.s have come from other countries, as well as being amplified in the U.S. Importation of cases will constantly be an issue when states like Florida are a hot-bed for the circumstance due likely in part to DeSantis political ambitions overweighing safety for the American people. Between instituting a mask-less requirement for all Florida schools and threatening district leadership with pay cuts if they try anything(and now that pushback), I don’t think we’ve yet seen the worst of his policies, as they continue to ignore evidence and enjoy cherry-picking data.
The U.S. C.D.C. messaging creates a specific narrative that does not help to eliminate the pandemic.
The current C.D.C. messaging focuses on pressuring the unvaccinated as the cause of V.O.C.S. and the reason for our current surges, which is a half-truth. The vaccinated, are, unfortunately, also spreading SARS-CoV-2, as much, if not MORE, than unvaccinated due to their larger numbers and similar lack of adherence to interventions; the difference is in how far that spread goes. The evidence regarding vaccinated folks carrying the virus has been known for some time; the initial SARS-CoV-2 virus had been shown to be transmissible among vaccinated, but far less than typical. We also suspected V.O.C.S. might change the game up. On March 10th, J.A.M.A. Viewpoint from the C.D.C. “A growing body of evidence suggests that fully vaccinated people are less likely to have asymptomatic infection and potentially less likely to transmit SARS-CoV-2 to others. However, further investigation is ongoing.” (Christie, 2021)
“The risks of SARS-CoV-2 infection in fully vaccinated people cannot be completely eliminated as long as there is continued community transmission of the virus. Vaccinated people could potentially still get COVID-19 and spread it to others. However, the benefits of relaxing some measures, such as quarantine requirements, and reducing social isolation may outweigh the residual risk of fully vaccinated people becoming ill with COVID-19 or transmitting the virus to others.” (Christie, 2021)
This is from a paper the C.D.C. director co-authored; the tone was already being set for the shift in messaging; however, what’s certain, was that we should not discourage interventions but relax measures according to regional outbreaks. California’s tier system successfully allowed counties to better control their circumstances; the lessons learned would have been easily translated, as they more recently have been in the new C.D.C. guidance.
But…following the strange shift to ENCOURAGING vaccinated folks to resume all activities without consideration for interventions was at the very least reckless. The medical blog site The Conversation echoed how most Public Health folks felt about this strange messaging. “Vaccines can be great at preventing you from getting sick, while at the same time not necessarily stopping you from getting infected or spreading the germ.” (Mishra, 2021)
We knew caution was essential to maintain because many suspected immune escape and viruses to continue to create potentially new V.O.C.s when the subvariants affect one another. We knew immune escape was a potential problem, we suspected increased transmissibility of new V.O.C.s, and yet not until weeks after Biden’s celebration regarding successfully not reaching 70% by July 4th and more information coming out about Delta did the messaging shift.
For those of you who are interested in high-value content regarding accurate information about COVID-19, might I suggest https://www.covidhealth.com/ and https://www.unbiasedscipod.com/ They put out lots of well-designed graphics and sharables like the one below.
from Unbiased Science Podcast
Important regarding the Delta V.O.C., The increased transmissibility is roughly twice as potent as the original strain, increasing viral load early on by as much as a thousand times higher. This not only indicates significantly more pre-symptomatic transmission, but importantly it improves the sensitivity of our PCR tests. Previously, PCR tests had a false negative rate which decreased to near nil close to day 5, but due to the increased viral load, Delta is detectable earlier than the original strain. Overall potentially improving test sensitivity by upwards of 10-15% due to the smaller windows of false negatives.
People were grossly unaware of the reality of the problem partly because the news doesn’t understand public health. Occasionally the NYT has been helpful regarding their data; however, their interpretations, opinions, and articles vary immensely based on its author.
This discourse was confusing for the general public because of media trash like this.
Made more confusing by choices like this from the C.D.C.: As explained in my previous article, the C.D.C. isn’t really looking for breakthrough cases, although the states are recording data on their own. Given the political climate, this *seems* not well thought through. It’s also important to note that breakthrough cases are defined by two weeks following vaccination, which puts partially vaccinated folks into the general lump. DEBLASIO, DID YOU READ THAT? Why the Capslock? Because the Mayor of New York City’s strange vaccine I.D. requirements only need one dose to count and may repeat the Springsteen debacle of vaccine nationalism, because what vaccinations count? L.A. reinstituted a mask requirement, which is…well…easier, more inclusive, and pisses off people who don’t want cloth on their face. The LA requirement also has no teeth, so most folks will and have likely ignored it to a degree, which we’ve been seeing alongside growing tourism likely importing cases.
But now the C.D.C. finally is on board with an actual solution, and of course, folks are doubting the agency…again. Do they deserve the doubt? Yeah, I’d say they tarnished the trust with the U.S., now multiple times over masks, so this was an epic fail on the part of the C.D.C. to do this, in this fashion.
But now that we do have reasonable guidance, let’s talk about how we should live with this pandemic.
We’ll get into the nitty-gritty of just why the C.D.C. messaging is so bad after this analogy.
Gritty is a mascot and the logo are owned by The Philadelphia Flyers
IT’S RAINING, MEN.
However you consider the Coronavirus/SARS-CoV-2/COVID-19/’Rona Pandemic, its essential to consider how a public health body should explain preparation for everyday folks.
We should think of SARS-CoV-2 like we do precipitation. Now, with better testing, better maps, integrated map tools into Google Maps, this type of analogy can make a lot more sense.
First, we have to look locally because that’s where the problem lies. A Pandemic in this sense is considered by its millions of regional outbreaks. So we can think of it as a massive Global super-Hurricane capable of producing all weather phenomenon.
Does it sound potentially terrifying? It should. Our toolbox of protection against rain may be raincoats, umbrellas, boots, maybe a towel by the door. For snow, we might need a snow shovel, salt, thicker coats, snow boots, etc.. We prepare for a pandemic in the same fashion, it’s just a little harder for some folks to initially see this because it’s a generally invisible threat.
The prevention toolboxes listed above are for an individual, and there are more for the community, and the State, should the weather become too burdensome on the individual. There are also toolboxes for response, maintenance/long term, and importantly for the future, meta-analysis, but let’s focus on what you can do, and maybe a bit about what some stuff around you can do.
These are the tools in our toolbox for an individual by importance:
1. Getting the Vaccine, in terms of rain( SAR-Cov-2), It’s like having a scotch guard bubble, one’s feet might get wet, and the bubble gets scratched up as it encounters things like hail(V.O.C.s).
2. Wearing a mask is like an umbrella, so if any water does get in, one is still dry to a degree, but one’s feet still get wet. (benefit is an umbrella can reduce the rain for others nearby, but don’t share masks)
3. Interactions are a combination of physical distancing and time. These are the boots, and how they’re used determines what type of boots they are and to what they’re resistant. The less time an interaction requires, the stronger those boots are, the greater the distance the interaction requires, the more protective those boots are. E.G., If an Interaction takes 15 minutes, and someone can keep a distance of 6-8 feet, that interaction previously ran a low risk but now runs a low but higher risk with Delta. It would be like wearing boots with worn soles a small hole in moderate rain; socks likely will get wet the longer the stay, and with random hail(V.O.C.s), it’s making the water splash about getting the bottoms of pants wet.
4. Airflow, often this can be considered Inside Vs. Outside. There are lots of ways to improve or increase airflow, opening windows, using air purifiers, increasing the cubic footage (typically heightening a room), adding negative pressure or exhaust fans. Each of them, like every intervention, mentioned, layers to add protection against SARS-CoV-2 and its V.O.C.S.
5.Hygiene isn’t just washing your hands. In this case, it’s cleaning your hands after you interact with things in new buildings or commonly touched items outside. It’s avoiding touching the face, nose, and eyes while not in the home. It’s the analysis of our washing routines to make sure we enter our homes clean, which can mean taking a shower after a long day at work if work is in a public or shared space with lots of people. Hygiene also reduces our risk of getting multiple illnesses. Some folks might wear lycra gloves to avoid constant handwashing, but they should rotate through sets as they go from location to location.
6. What? There are more tools?! What else can we do? Vote for political candidates who aren’t actively telling others not to or disable their ability to do any of the above. Really. This is by no means an endorsement of any political group; it’s just common-sense Public Health. Leaders who broadcast and elect to enact policy making an outbreak easier are objectively a bad choice during a pandemic.
7. Hah! There’s even another one, because the Internet. Correct misinformation to the best of your ability, even your own. The Scientific Literature is constantly growing and correcting itself, and when agencies interpret this, once an Administration is involved, it has to consider what obligations or national temperament may require. This is part of why C.D.C. Director Walensky removed the mask requirement because it would release tension regarding intervention compliance, giving a break, for what she would have likely suspected, was a wave coming in the Fall. The likely additional guidance by the White House to disregard all interventions once vaccinated was likely weighed with the unknown of Delta. The Literature expanding to include the significantly higher transmissibility put pressure on the C.D.C. to install the current system, one which always should have been the guidance. But Literature doesn’t guide every government decision; there are a lot of data to consider, including compliance with interventions. So government agencies have a degree of fallibility here. But it’s crucial that when we correct misinformation, we shouldn’t be a dick about it, speak honestly, but withhold that new Government Encouraged Outrage.
For a moment, to see how the messaging is doing to improve vaccinations, let’s return to the K.F.F. Vaccine Monitor to see what stalwarts likely remain, besides those of us with chronic conditions who require the timing to figure out when to vaccinate or who simply cannot given the current guidance with their doctor. We should assume that the vast majority of them would likely answer “Wait and See” and a few as “Definitely Not”, but not enough to break 4-5% and 1-2% respectively of the whole. So about 20% of Americans still leaves many folks who aren’t interested in vaccine-induced immunity for whatever reason.
But the most compelling thing from this month’s K.F.F. Vaccine Monitor was this unsurprising comparison “News Of Coronavirus Variants Has Caused Some Adults To Change Behavior, Two In Ten Unvaccinated Adults Say It Has Made The More Likely To Get Vaccinated” vs “A Majority Of Vaccinated Adults Say News About The Possibility Of A Booster For The COVID-19 Vaccine Hasn’t Caused Them To Worry About COVID-19 Protection, Black And Hispanic Adults Slightly More Concerned.”
These data illuminate that the white house messaging DARING folks to get vaccinated to avoid creating V.O.C.S. and blaming them for the new surges aren’t having the desired effect of increasing demand for vaccination.
So it’s time to consider what’s next. The increased vaccine employer requirements are absolutely squeezing the “only if required” crowd down to zero. Still, the remaining potentially 15% by the end of this year who will be Choice Unvaccinated might be enough to continue this nonsense for another year yet, instead of going from mitigation to control like in New Zealand or Taiwan.
How do we convince the stalwarts? Talking to them helps, but only when it’s productive and informed.
A big thing, though, is honestly, ignore the big fluffing. The thought-leaders encouraging anti-vax thrive on being the underdog and defending their position, don’t give them clicks, just brush it off like the nonsense it is, and also don’t feed the hating on them, ya know, like the U.S. C.D.C. messaging inadvertently does.
It’s important that we all agree on something here, though, that no one deserves COVID-19. Leaders do bear some responsibility; however, that doesn’t mean someone deserves a life-threatening condition that could result in a chronic illness or death. If we want to get through this pandemic, the only way we can is together.
By considering the Interventions relative to the danger around us, much like we do with weather every day, we can best take caution to protect ourselves and our communities. We may not always need to wear a mask all the time, but when the risk is high, we should take as many precautions as possible and use as many tools as we can carry.
Get Vaccinated when/if you can. Wear a Mask indoors, in crowds, and in mass transit. Also, consider the other tools as the situation demands.
References
Christie A, Mbaeyi SA, Walensky RP. C.D.C. Interim Recommendations for Fully Vaccinated People: An Important First Step. J.A.M.A. 2021;325(15):1501–1502. doi:10.1001/jama.2021.4367
Lazarevic I, Pravica V, Miljanovic D, Cupic M. Immune Evasion of SARS-CoV-2 Emerging Variants: What Have We Learnt So Far? Viruses. 2021; 13(7):1192. https://doi.org/10.3390/v13071192
Levine-Tiefenbrun, M., Yelin, I., Katz, R. et al. Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine. Nat Med27, 790–792 (2021). https://doi.org/10.1038/s41591-021-01316-7
West, S. L., & O’Neal, K. K. (2004). Project D.A.R.E. outcome effectiveness revisited. American journal of public health, 94(6), 1027–1029. https://doi.org/10.2105/ajph.94.6.1027
As of June, 2021, I will have been eligible to get the COVID-19 vaccine for over four months now as a Solid Organ Transplant Recipient. I am a person who received a liver transplant, younger than the average at the age of 35. My transplant journey is a rough story concerning my life-long battle with Hepatitis C, six treatments, and six plus years in End-Stage-Liver Disease you can read more about the story here.
Because this story isn’t about me, per se, but about the circumstance that I find myself in, along with so many of my peers. Before I explain further all of this, some background is in order as to explain the importance of understand the nuanced differences in vaccine hesitancy and folks who are among the “unvaccinated”.
I belong to part of a large group of vulnerable folks, collectively, spoonies is the best term here. Because the complex mix of auto-immune, genetic, medically induced and viral infection induced immune responses include lots of folks. From folks with certain cancers, folks with HIV, to folks like myself who take medication which suppresses our immune system.
Collectively it’s estimated that we comprise about 4-7% of the United States population, with about 2.7% of the population being transplant recipients like myself.
Many of us who might benefit less from the vaccine, will continue living as if nothing has changed. Masking regularly indoors, outdoors in groups, increasing our hand-washing and keeping some physical distance from others, especially if near crowds, and minimizing interactions.
There are many estimations of when Community Immunity may take hold, somewhere between 70-90% is the average of all the literature and articles I’ve come across. In Brazil, the efforts to induce natural herd immunity, in part by relaxing non-pharmaceutical interventions like mask wearing, resulted in the population of Manaus having as many as 76% of the population infected, and also provided us with the P.1 Brazilian variant now being referred to as the Gamma variant. So to be at the the functional level needs to rely more heavily on vaccine induced immunity, in part because it potentially lasts longer. More importantly it is more robust than natural immunity as more documented cases of reinfection have occurred through natural immunity, especially in regards to Variants of Concern. And it slows the potential for new variants due to significantly reduced levels of viral procreation when vaccinated. (aka less viral load in vaccinated folks means less potential for evolution into new variants, because it doesn’t generally evolve in the wild, just in people/animals.)
As Variants of Concern continue to appear due to the uncontrolled and widespread state the pandemic is currently in, we must consider that these will eventually impact transmissibility of SARS-CoV-2., as both the Alpha variant (AKA UK variant AKA B.1.1.7 variant) and the Beta(AKA South African Variant AKA B.1.351 Variant) have. How this in turn is met with growing vaccine uptake, time is slowly revealing.
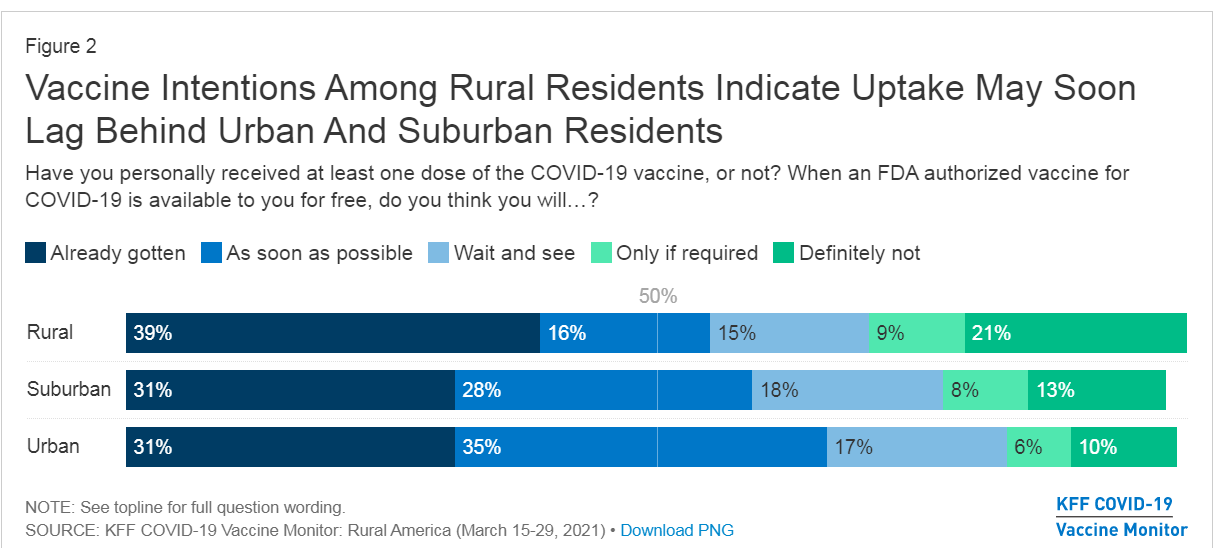
For those not familiar, this is the Kaiser Family Foundation Vaccine Montior. An important constant pulse on vaccine uptake and trends here in the United States. Crucially, it has been monitoring the Already got it vs ASAP vs Wait and See vs only if required vs Definitely not.
Within the Spoonie communities some of us may attempt to get the vaccine, anecdotally, many who have reported higher than average instances of side effects, or no effect whatsoever. For others in the Solid Organ Transplant situation concerned about the vaccine check this out, it won’t help you make your decision, but it might help inform it a bit more, especially if you check their references.
Now for the reference to the title of this piece, who are these captors? The vaccine hesitant for non-medical reasons, and most importantly those who would refuse themselves and their children the safety of a protective vaccine.
For spoonies like myself who long for a return to seeing friends and family, going to a graduation, a wedding, even a funeral, there is little hope in reaching community immunity without the help of those who also fall into haven’t gotten the vaccine category. For veterans of the spoonie community, we’re no strangers to phonies, con-artists, scammers, and conspiracies, especially on the internet, not to mention the people who call them out, and people who accidentally call out real Spoonies. When you achieve a certain level of fame on Instagram, some spoonies find themselves fighting off fake accounts, copies of their own who grift unexpecting folks. We’re used to folks pretending to be disabled standing next to us in line for a Disability Access Pass in Disneyland, or folks who claim medical exemptions for hardships where none exist. And we’re used to the increased scrutiny and disbelief of our condition if not visibly apparent. For some it reinforces imposter syndrome, it encourages them to avoid seeking help, there are layers to these problems which are important to know exist as we explore the reality for folks like me in 2021 in regards to vaccine hesitancy.
The alarmingly high number of 13-15% of folks answering definitely not to the vaccine likely includes a small portion of folks like myself to more extreme cases who absolutely cannot get any COVID-19 Vaccine. But even without considering that, we can be assured that this % is not consistent state-by-state, and significantly different between rural and urban populations.
We see that among rural populations, the majority of folks who would not be vaccinated number as high as 21% on average. It is impossible to extract from this data where spoonies might fall. Because some of us have already gotten the vaccine, many like myself wait and see, and some already know they cannot take the vaccine, or are so alarmed by side effects they’ll only do so if required, and even then they may quit or be fired.
Let’s assume the upper limit of 28%, a stat where every spoonie cannot vaccinate, with a lower limit of 23%, where only a few spoonies vaccinate successfully against SARS-CoV-2. It means that on average among rural populations the vaccination rate might not breach 72-77%, clearly around or below the 76% which existed in Manaus for their attempt to gain Herd Immunity. Again, Vaccine Induced immunity is likely stronger against SARS-CoV-2 and its VOCs, but at such low rates of vaccination, it poses a significant danger in a different way: Reservoirs. Reservoirs (of infection) are individuals, animals, plants, substance, soil or a location which the virus lives and multiplies. Reservoirs make it hard to eliminate an epidemic, in the U.S. and other countries the prison system does this with Tuberculosisand Hep C. As populations in the prisons have significantly higher incidence of disease than populations outside prisons. Reservoirs don’t’ work well if those folks aren’t intermingling but unfortunately…
Another chart form KFF tells us why, unfortunately, most folks who are won’t vaccinate know one another.
Note the highest groups are among Republicans and Evangelicals, collectively amounting to more than 40% of either not vaccinating or needing for it to be required. It is likely that many of these folks attend the same churches, belong to the same or nearby communities, and will otherwise engage with significantly less regard or no for interventions like mask-wearing, social distancing or extra hand-washing. (46% according to the same KFF Vaccine Monitor) Making it more likely that if they are infected, that they may spread it to others who are also not following interventions.
We’re familiar with this problem it exists in the US in a variety of ways, In 2017, Minnesota’s Measles outbreak was due to a Somali-American community being fooled into opting out of the MMR vaccination. Granted, the vaccination rate among the group was as low as 41% among children, its important to consider that outside of this group the vaccination rate is likely near 95%+ for neighboring communities. If the community intermingles with other anti-vaxx communities they bear the risk of spreading it further, or worse trading it back and forth between groups who are similarly unprotected against the virus.
The reality of new cases going forward is this, in Seattle early June 2021, they found that 97% of cases had occurred in unvaccinated folks. It’s worth mentioning that when vaccinated the likelihood of symptoms and severe COVID-19 is significantly reduced due to it being a protective vaccine, so it is highly unlikely that even if a vaccinated individual came down with symptoms that they might even go the hospital or even be tested without a severe response. In addition more folks with less severe symptoms are less likely to be counted among cases as they’re likely staying home following best guidance.
That being said, it means that unvaccinated folks are where the virus will live, and where it will evolve, and the tight-nit anti-vaxx communities are ripe for being reservoirs.
With this information in mind, lets revisit the title again: When captors masquerade as allies.
The Fault in our Stare Decisis
Anyone paying attention can clearly note that folks who might be vaccine hesitant, by nature, aren’t necessarily allies to Spoonies who live with health conditions limiting their daily lives.
When someone with a health condition needs accommodation to be able to enter, use, or otherwise act in an equitable legal fashion in a public space, or space available to the public, the ADA is often invoked. When someone is employed, and an employer seeks to unfairly punish an employee due to the specific conditions or imposes requirements which make the employee unfit for their role, the ADA can be invoked. If you’re interested in learning how the ADA came about, it’s a ton of activism.The Americans with Disabilities Act is a tool for folks with legitimate disabilities to help the world become a more equitable place. It allows folks who might otherwise be excluded, an opportunity to be included. Additionally, another law often utilized by Spoonies, patients or folks with disabilities, is Health Insurance Portability and Accountability Act or HIPAA. For school children FERPA might also apply, but that’s a whole ‘nother bag of worms. HIPAA protects records from being used against us, by securing them, otherwise it would be likely that employers, insurance, and even hospitals themselves might use this data is other ways. By securing privacy of health information, It prevents stigmatized conditions from discrimination, prevents insurance from specifically coordinating with the employer to charge you more, prevents hospitals from profiting off the data by selling it to pharma/med device/tech companies. You don’t have to disclose your health status, because of a complex interpretation of the constitution by the Supreme Court regarding the right to privacy, but it won’t help getting out of wearing a mask or not being asked about vaccination status. Specifically Griswold v. Connecticut (1965), Eisenstadt v Baird (1971), Roe v. Wade (1972), and Lawrence v. Texas(2003) are generally the cases which really cement the Right to Privacy.
These two laws, in concert with the Stare Decisis (Court Opinions regarding legal situations involving these laws which expands or modifies their interpretation) of courts in regards to them, create the legal shields which help some folks stay employed, work, live, seek education, or simply interact with the world.
As many who might want to ignore rules for their own personal reasons, might seek to misuse these protections, to shield themselves from responsibility. Over the year+ of this Pandemic, multiple different clearly fake cards have been produced claiming that these two laws would allow the bearer the ability to ignore Public Health protocols being privately enforced by businesses, or publicly enforced for national security, when they most certainly do not.
While they might wield the ADA and HIPAA like a club, they masquerade as folks who need it. Now, as the vaccination effort approaches a critical juncture, we see this same poisonous-allyship. To avoid personal responsibility, a handful will pretend to be spoonies. But even when they do not masquerade, the reality of their not taking the vaccine means a lower likelihood of community immunity, and they remain captors of folks who have no choice in the matter.
I wish this were the end of the part about anti-vaxx co-opting of the “unvaccinated” category, but sadly TikTok has become a strange place for anti-vaxxers to have a new trend. From the hunger games “I volunteer as tribute” phrase and salute to even using the mocking Jay whistle. This is much like the opposite of those attempting to masquerade as allies, but here instead as unvaccinated spoonies being lumped in with their “solidarity” for being unvaccinated. For Spoonies who have no other alternative to being vaccinated, or for Spoonies like myself where the vaccine is less likely to work, this is beyond insulting. We already advocate for real health problems, we don’t need this weird diversion of focus.
As spoonies we must wait for community immunity or the virus to become a minimal threat and no longer endemic to a region. Both of those are tall orders right now given those who would masquerade as allies are now effectively holding us captive, as for many of us spoonies with immune-issues will continue on as if it were still rampant, for we were the vulnerable population before the vaccine’s availability, now we could end up being even more so.
Unfortunately last month the CDC announcement of their new mask guidelines began a terrible trend. The CDC recommendation ignores evidence of transmission from vaccinated folks being similar to that of asymptomatic cases.Why is that concerning?
Asymptomatic and pre-symptomatic cases have been the dominant method of the last year for transmission. ” transmission from asymptomatic individuals was estimated to account for more than half of all transmission” This predominantly due to our minimizing interactions, use of symptom checkers like thermometers, and mostly because folks who felt ill were told to stay home and given additional sick days to accomplish this. So now, as we move about again, and the majority of folks, functionally become like asymptomatic cases, are less likely to be tested because they are vaccinated, and are less likely to feel unwell, prompting less caution regarding transmission. Public health experts have repeatedly gone out of their way over the past month to explain the necessity of these masks after vaccination, and a recent study highlights these points. And with the data that we’re seeing here, with so many folks not vaccinating, The CDC mask policy only makes unvaccinated folks more vulnerable. So to see that Cal/OSHA, Newsom and the lot of them caved again to “business leaders” AKA Big business is absolutely unconscionable for a number of reasons. And to cave in an odd way, to no longer recommend that workers, even in high-risk jobs, wear a mask is likely due to additional pressure from the recall campaign.
1. Pandemic still raging around the world, importation risks remain high, especially with new VOCs.
3. The tests still kinda suck! Due to the windows of false negatives no current test breaches about 60-80% in sensitivity aka false negative rate. The problem is the way the virus does it’s thing compared to the administration of the test on the patient timeline, some more sensitive tests exists, and saliva testing has shown to be more robust in early detection than more typical NP/OP swabs.
4. The CDC mask guidance dropped months earlier than it should have, using them as guidance to make things consistent has nothing to do with health, rather with consistent regulation showcases our Safety 3rd mentality regarding health regulation.
5. When we consider the rates of potential folks who cannot vaccinate alongside the folks who will not, these numbers make community immunity potentially our of reach, especially with continued importation of cases, which can see more clearly with VOCs. All of these decisions seem quite premature.
In situations like this, caution is the better decision, moving slowly, with available data.
Right, Rick, but how does this affect you personally? I’m a transplant patient, who is planning my vaccination with my doc, it means waiting more than I’d like, it means seeing those around me start to engage in a slowly opening world. It means saying no to networking opportunities, potential career-boosting opportunities, and a great deal of advocacy. It means having limited interactions with friends and family even though the vast majority are vaccinated. Having close family members who are also in the same Spoonie boat, increases our vulnerability. I’ve already spent 6 years in end stage liver disease and the last year damn, I know the fear and potential pain many in the community sense or feel. Unfortunately the vaccine may not even take due to my immunosuppressant meds and in the rare event that my antibodies are detected, it is not recommended as a confirmatory test on immunity.
But while SD county only has about 19% of its population unvaccinated currently, neighboring Imperial County has about 32% of its population currently unvaccinated. You san see County by County data here.
Red represents conservative leaning counties, San Diego still slightly leans conservative.
These percentage points, combined with the reality of growing interstate travel and vacation use, means as a tourist destination, San Diego is also likely to see more importation cases from neighboring states with less regard for health and safety. So while San Diego folks are more cognizant of their health, tourists might not be.
Okay, well that was awful, is there anything that can be done? Or are we just fucked?
I mean, for those of us in the spoonie community, we know how common the latter is, but in this case there is more that can be done. While states give away money, or Xboxes, cars, or whatever else seems clever, the reality is that folks who aren’t interested aren’t likely to be swayed by a SWOT analysis. They’re likely to be influenced by their peers. Some “Maskueraders” won’t understand so easily and it may take time for them to understand the real risk and adjust their worldview. Patience and tolerance is important.
If we want to be free again in this country, in this world, we must be prepared to protect our community, our nation, and our world, by at the least getting a vaccine for COVID-19. It probably would also help if the federal and state governments could agree on a standard for ensuring vaccination, like having some kind of universal database (it exists with HHS already it’s just not connected to anything outside of a few departments) having at the very least a robust nationwide Electronic Health Record system would help in every health fight, improve mobility within systems, reduce administrative costs, streamline costs/billing and further the goals of health equity in the American population.
In the meantime, please wear a mask when around others in close quarters, or in mass gatherings/mass transit, and if you aren’t yet vaccinated and can get it, please do and encourage friends and family to do the same.
TLDR: Vaccine rates won’t go down unless we talk to our friends, family and neighbors and make sure everyone who can vaccinate does. The CDC Mask policy makes the pre-emptive reopening potentially worse, and worse for unvaccinated folks who account for nearly all cases in the US. Anti-vax folks pretending to be disabled doesn’t help anyone. Blending the category of unvaccinated conversationally benefits anti-vax movement, as they pretend to be martyrs (who don’t think they’re going to die? it’s confusing) Expanding poor health policy only further erodes what little public health trust exists in institutions. We can always hope it’ll turn out alright, but as a six time survivor of Hep C treatments, my caution regarding Epidemics is imbedded.
Johansson MA, Quandelacy TM, Kada S, et al. SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA Netw Open. 2021;4(1):e2035057. doi:10.1001/jamanetworkopen.2020.35057
La Marca, A., Capuzzo, M., Paglia, T., Roli, L., Trenti, T., & Nelson, S. M. (2020). Testing for SARS-CoV-2 (COVID-19): A systematic review and clinical guide to molecular and serological in-vitro diagnostic assays. Reproductive Biomedicine Online, 41(3), 483–499. https://doi.org/10.1016/j.rbmo.2020.06.001
Patel MD, Rosenstrom E, Ivy JS, et al. Association of Simulated COVID-19 Vaccination and Nonpharmaceutical Interventions With Infections, Hospitalizations, and Mortality. JAMA Netw Open. 2021;4(6):e2110782. doi:10.1001/jamanetworkopen.2021.10782
Often have I searched the internet wondering, where can I find helpful Hep C resources now that HCV Advocate is gone? Well there’s HepMag, Help4Hep (if you need help with treatment give ’em a call!), IhelpC, and HepatitisC.net, but they’re really good tools for information or story sharing, or delicious liver friendly eats(IHelpC). To help provide a space where we can connect with others who have experienced Hepatitis C Virus (HCV) or those who seek treatment, advice, guidance, or want to do more in the community!
This is the HCVME Community Discord It will prompt you to create a discord account. Due to the public nature of the discord, I have required a registered Discord account. Additionally I’ve set up a channel which features the latest from twitter regarding Viral Hep and Liver disease. featuring advocates like myself, but also liver organizations and medical experts. I’ll be on there posting HCV resource information and what not periodically. and come June, I’ll be on the discord regularly for chats! Please join us! make sure to agree to the rules and pick a role with fits you!
In May we’ll be launching the HepChat Hour on Monday evenings Pacific time 5:00pm-6:00pm on the HCVME Community Discord!
We had just wrapped up a three day conference for Help4Hep, and I was wearing a shirt, a shirt I originally wore for a press conference against the BRCA.(The awful replacement for the ACA on the senate floor last year.) A form fitting black cotton T-shirt that reads: “Hello, My preexisting condition is Hepatitis C.” The shirt’s purpose was to bring to people’s attention two things: One that Preexisting conditions aren’t really visible, but they are common, and Two, That Hepatitis C is among them, and I have it. Even while being cured of Hep C, in the eyes of the medical world and insurance I will forever be a Hepatitis C patient.
Maybe it was because I was standing alone before we boarded, maybe it’s because I was visible, sitting in the front, but regardless why the next series of events happened, it’s unfortunate that they did.
I wear a mask because I’m immunocompromised due to Liver Transplant
I was seated in the front row, and I was talking with the lady seated next to me about hepatitis C. My shirt was a conversation starter, earlier I’d explained the prevalence and the cure to a few others who’d asked. She was explaining to me that her mother had it and we spoke about the cure, to which she seemed surprised, but often people are unaware of it, so I went into more detail. I explained that there’s a lot of ignorance around the virus, and the cure, largely due to stigma about even talking about.
“Excuse me sir, I’m going to need to talk to you.” The flight attendant interrupted. He and another attendant pulled me off the plane and onto the boarding ramp. he began ” A passenger expressed concern about your shirt, could you explain?” Without thinking I responded I’m a Hepatitis C advocate, I just came from a conference. Noting their faces unchanging waiting for more information I continued. There’s a lot of ignorance about the disease, and a large part of that is due to stigma, so I’m not surprised someone is concerned. They asked if it was an issue.
And I responded, unsure if they meant an issue for me or for them, as the situation implied they took issue. “It’s a blood borne pathogen, it’s blood to blood only,” I continued, still waiting for a response I explained that I was cured last year, but regardless this shirt is my status, and it’s not an issue. I’d had enough of their concerned faces, and turned around and went back to my seat.
I was far too aware of the level of control airlines have over passengers, and now being a transplant patient I only had so much medication with me, so being stuck there was a concern.…
But across all of my online dating profiles I will openly disclose that I have HCV along with pertinent information.
My virtual identities which I once held separate I’m going to link.
I don’t really know what will happen.
I don’t know how people will take it.
But we’ve all got our shit.
In addition to doing the ongoing dating series…
Next month The Five will be available to read in it’s first iteration in six parts.
It is an introspective look at the previous treatments’ failure and how to fail best.
(like Astronaut Chris Hadfield says “Visual Failings, not Defeat” )
As May is coming up, I wanted to highlight the amazing changes that have happened in the past year when it comes to treatments and the bright future there is for those with Hepatitis C.
Of the daunting challenges to overcome, awareness can help address one of the largest ones. The fact that the majority of those who have the illness will go unaware until they begin showing symptoms and by then permanent damage can already be done.
It’s easy to understand why this can be a terrible idea, but considering 1 in 20 Google searches are medical related it’s not hard to understand why it was done.
For those of you not hip web-lingo, it’s a scraper. Scrapers copy content and aggregate data onto one platform, typically a website, however recently apps have become fantastic at using scrapers.
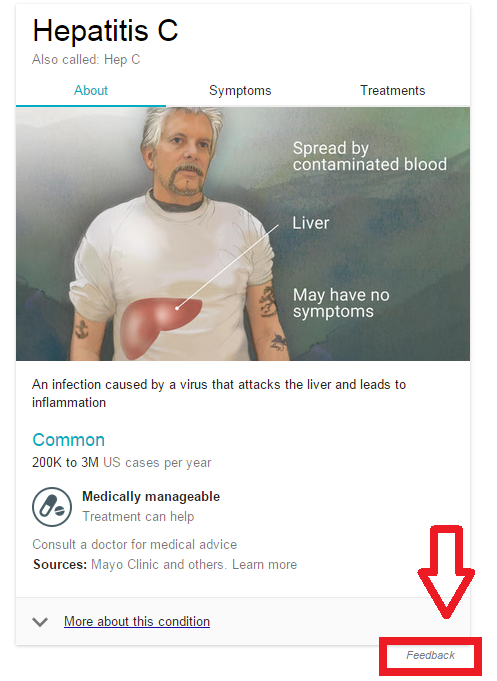
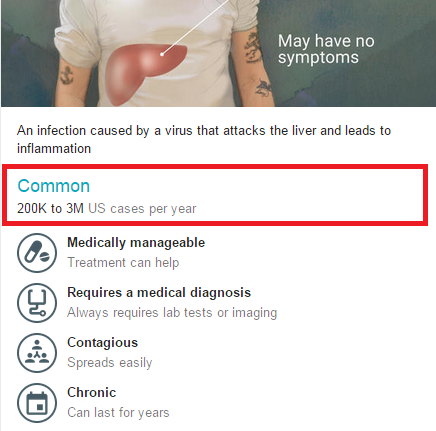
Let’s look at the 4/12/15 Google high-quality image medical data for Hep C.
This has recently changed from sexual contact to spreads easily.
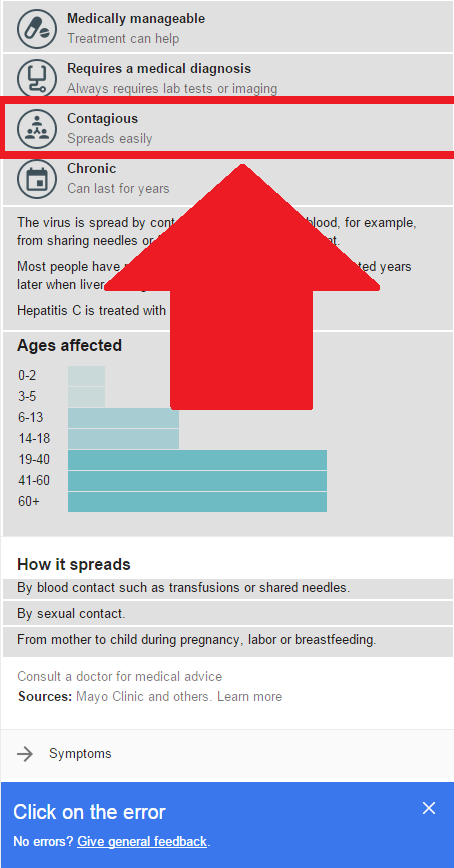
I can see a glaring issue without having to go much further. Under contagious its top listing says that it’s Mainly spread by sexual contact.
The main methods of transmission are in order: Intravenous Drug Use, Transfusion (in the USA prior to 1992, in Canada prior to 1990), and needle stick/Health care worker exposure.
This is the principle problem with scrapers. Even it grabs the data properly, Sexual intercourse using has the longest section when describing the transmission methods…why?
Because there is a lot of controversy around it. The most recent poll was done by the CDC in 2010, and the questions that were asked, were fairly direct. Even in other polls that have come out through the years, this issue always comes up: The biggest section of the Hep C population consists of Intravenous, mostly illegal, drug users. It’s far less damning for someone to claim to have received it sexually than via drug use.
When studies have polled HCV patients directly, usually through a doctor, they find slightly better information, which is why we have such an interesting spread of information. They also have been examining the virus, to see how likely these claims could be. E.G. looking at the life of the virus outside the body, looking at how the HCV RNA in sperm is typically inert or non-existent. (it’s around 9% of the HCV infected male population that have it, and less than 20% of that 9% excrete enough for it to potentially be transferred) The less likely means of transmission as in order: Vertical Transfer: Mother to Child (it does not go father to child), Personal items (nail clippers, razors, etc..), Sexually can even further be broken down: Rough unprotected anal intercourse, rough unprotected vaginal intercourse, unprotected intercourse/rough intercourse. It is not simply by means of sexual contact, which is a much larger category.
Okay Google, now…let’s talk about how we correct this problem. There is a feedback button at the bottom for correcting mistakes.
But this is also terrible, because most of the time people who Google ailments and diseases are usually anything but experts. So the idea that an under/uninformed user is going to be able to use that feature is silly, at best. In fact, many who use this method, may reinforce what Google says by repeating their new-found knowledge to others who are under/uninformed.
The feedback method is used a lot by Wikipedia. And the correction method works for Wikipedia because often times authors/experts will correct the information using verifiable credentials. But even still, Wikipedia’s accuracy is at the mercy of its users.
The other issue with this new presentation of information is the listing of sources. Google is borrowing the credibility of the top websites in its scraper. The Sources listing as “Mayo Clinic and others” uses a recognizable name to help a user view this information as accurate. Additionally there is no list, of what these sources area.
Ethically it should list sources, as “Sources” and not disclose any of them until the user checks the sources themselves.
While yes Google consulted with the Mayo Clinic, clearly not for that medical data, which is what makes this tool so useful. Not only would it allow Google a better idea as to how many of their users trust this quick medical information, but it would also allow Google to randomize the presentation of sources to encourage users to verify the medical information.
Why? Because if you see Mayo Clinic, 9GAG, WebMD and Top Ten medical facts about DISEASE YOU GOOGLED listed as sources, chances are you’ll look at the info with more scrutiny. Since then, Google has changed the main transmission method to “Spreads Easily.” Which, as a blood-born pathogen is far from the truth. Please Google Hep C, and help correct it. Also if you’re a medical professional, please help correct the information you know to be false. And please ask your Doc/Specialist(s) to help correct false information as well.
While there is a lot of medical information on the web at your fingertips, always tread with caution. Incorrect information, or half-cocked information should never be used for diagnosis. The internet can provide you with the questions you need to ask, the help of communities, and other resources to get help.
Misinformation for medical information is potentially deadly, and after all the internet is mostly a series of tubes.
Step 1: select the feedback button at the bottom of the app.
Once you’ve selected the feed back button it’s time for Step 2.
Step 2: select the “contagious” category highlighted above.
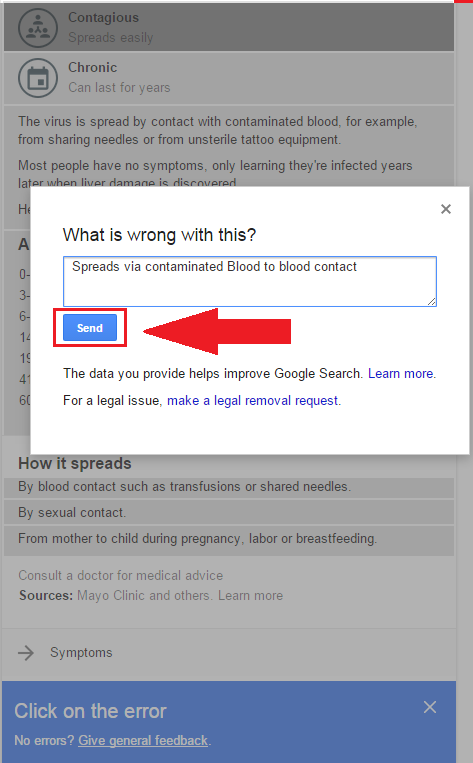
Step 3: Once you select that category a “what’s wrong with this?” will prompt. Please enter “Spreads via contaminated blood to blood contact”
Step 4: Select/click send!
Once you’ve clicked send, this message will display confirming you submission!
And Voila! within a few seconds you’ve just helped correct a major problem! There are two more sectors with the same issue however… there’s still more incorrect info.
So please put: “About 22k new cases per year, 3.2 million Chronically infected persons in the US.”
Under Treatments tab,
The Prescription category :
“Simeprevir rarely used in US. Should be sofosbuvir/ledipasvir (Harvoni) or ombitasvir/paritaprevir/ritonavir + dasabuvir (Viekira Pak), with or without ribavirin”
With the CND underway and news about ACA/Obamacare, A lot of healthcare related issues are on the table, nationally and internationally. If you’re interested in keeping tabs on what’s going on with drugs/pharma and all things narcotic internationally i highly suggest checking out the blog, or if you want something easier to digest check out the twitter hashtag #CND2015.
But as for the ACA/Obamacare… Let’s talk Healthcare Insurance.
Healthcare basics: Healthcare as an employee (which is the most common way about it in the united states).
Insurance and compensation are part of the bargaining agreement between you and your employer when you start working for them.
Insurance is a weird thing, but ultimately the employer is giving you a discounted insurance plan in lieu of other financial compensation. There are some companies that will pay you to opt out of their insurance, because it’s cheaper for them as long as they meet their units needed for group discount.
So when you get handed a dozen options from your HR department come fall, I’m sure you’ve noticed a few plans are ridiculously expensive. In some circumstances companies have executive plans which cover more than the options you were given.
Your pay-grade usually determines the allowance you get to buy a healthcare plan. It would be prudent to know that the ACA is the first real legislation to present a progressive tax system that extends to this compensation.
Why should you give two shits about all of this? Understanding benefits negotiations is as essential as negotiating your wages. Since it’s such an information disparity, most potential employees do not know what they’re going to get until they’re hired. It’s always good to know what insurance plans are offered by a company and how they compare to other options.
It’s also often the case that you may find that your doctor is no longer covered when you switch employers, even if it looks like the same plan. That’s because Healthcare plans usually have a list of doctors within their program. There are some medical groups that have associated healthcare insurance to alleviate this issue, and in a sense compete over your care without your say.
The necessity of Insurance.
Health insurance since the early 80s has been a rapidly growing part of paying for a hospital bill. Insurance is and always will be an all or nothing deal. Whenever Insurance becomes part of a marketplace it sets group rates and raises prices for those without insurance. This alongside Pharma patents, costs of medical equipment, and a disturbingly small pool of workers has helped to create some of the unusually high medical costs we see today.
Because healthcare insurance has become part of an employee’s compensation, healthcare is more often the primary means of payment for most medical groups. The employers bargain with insurance companies for rates and plans, those insurance plans present proposals to medical groups. For the most part the conversation regarding what you pay for healthcare is never up to your needs, and the services you choose from are what the companies have agreed upon. Limiting your choices as a healthcare consumer.
Exchanges allow for consumers to pick plans they would have otherwise never seen. Their major limit is their geographic region. If you’ve used Covered Ca, Healthcare.gov or even a private exchange you’ve seen how much better many of those options can be.
Payment without insurance is always higher, and if you’re savvy you might be able to negotiate a payment plan with the hospital’s billing and/or finical assistance dept.
But regardless you’ll pay more. This is one of the fundamental problems the ACA attempts to alleviate. The reality that if you’re employer doesn’t give you benefits(usually not fulltime), underemployed, or hanging income-wise out between 17k and 40k per year: you simply go without insurance, and risk falling into serious debt/health problems when something bad happens health-wise.
It also alleviates the issue of employer based competition by opening up the markets to consumers via exchanges.
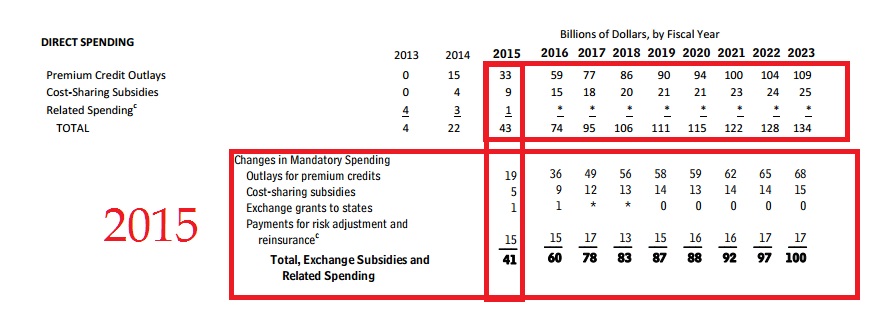
In our modern society, being so close quarters and risking illness/injury daily, it is necessary. So… I guess I should get to why I’m on this subject right now. Well, the reason I’m talking about this is because this last week the Congressional Budget Office announced its projections for 2015. The ACA (Obamacare) has a very interesting track record.
While there are a lot of disagreements as to why these changes are occurring and how it affects us, esp. with King V Burwell presently in the Supreme Court. To insure our health as a nation, the subsidy is an important factor alongside the exchange.
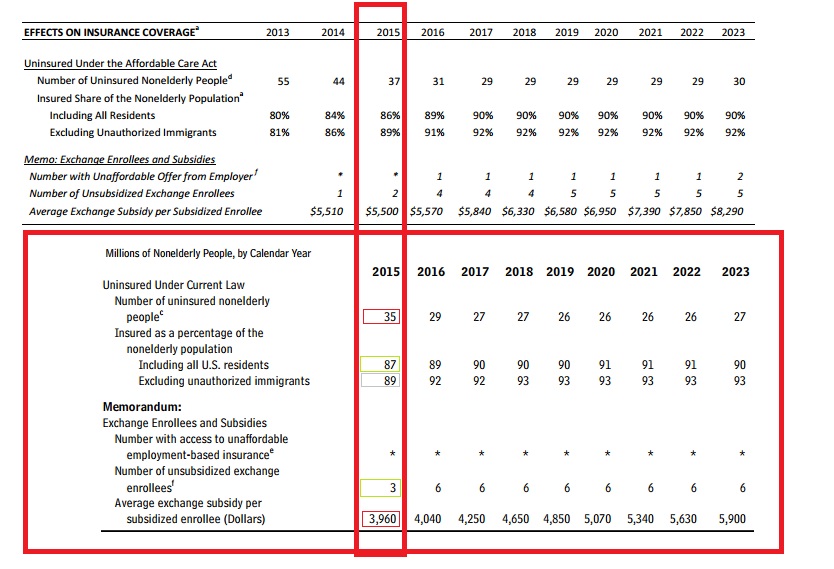
What’s noted here are some relevant facts: Affordable Care Act(Obamacare) will have lower projections in terms of cost and number of people covered using the exchange.
And these are the real changes in 2015
In order to better illustrate the exact changes, I’ve made some comparison charts using the data from the Congressional Budget Office:
Table 1
Here’s the neat bit of all of this, since we’re halfway between a census it’s hard to have spot on population projections, but 6 million less non-elderly people than projected is a doozy. With projections the relationships between the numbers are important. The goal of the ACA was the lower the number of uninsured. Expanded healthcare to 26 under parents plan, lower of full-time work requirements, the subsidy/exchange program, and 400% poverty wage definitions helped this relationship are all parts of the ACA that help accomplish this.
Table 2
As Table 2 illustrates there is a drop of enrollees in exchanges and Medicaid. There is also an overall shrinkage of about three million people. Two things will change these numbers over time: As states allow their constituents to use exchanges, and as signing up through an exchange becomes more user-friendly we’ll see better reflections.
While politicians bark at each other, the key to keep in mind is the relationship between the numbers.
Those signing up for exchanges vs. less uninsured is nearly the same (13/20) 65% for 2013 projections while (11/17) about 64.471% for real 2015.
This relationship implies the success/failure of the exchanges as it relates to helping those who are without insurance, in comparison to projected numbers. The numbers are not much different..
Those benefiting from the ACA’s exchange and expanded Medicaid definitions also are very similar from 2013 projections (20/24) about 83.33% while 2015 real (17/21) about 80.95%.
This relationship implies the success/failure of the ACA’s exchange program and expanded Medicaid definitions, in comparison to its projected numbers. Within one year, a little more than 80% of the United States’ uninsured population gained insurance they otherwise wouldn’t have. It’s actually more than that, but the table 6 has more data to better reflect that question. This number is a close expectation of the direct effect of the program.
Table 3
These are the big numbers most people are talking about regarding the success of the ACA/Obamacare. that overall Costs are down. Woohoo! Just Kidding. It’s really not that big a deal, spending allocations are very hard to project without a few years of historical comparisons.
Table 4
Again, Table 4’s numbers reflect the overall shrinkage in projections for 2015 vs. actual. This is just a more in depth table of where that exchange enrollment from table 1 looks like. What’s important to note is that more people signed up who are unsubsidized than expected. Realistically this implies a success of offering exchanges to consumers, rather than the importance of the subsidy. This implies that states not allowing exchanges (state by state means that it’s plans better reflect their constituents) penalize their residents by lack of consumer choice at the very least.
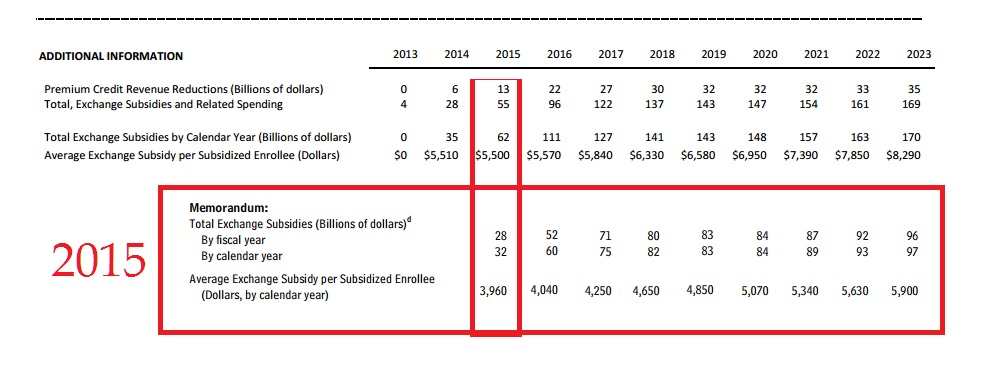
Table 5
If you want to count a huge success of comparative projections… it’s right here: Spending per enrollee dropped, by $1,540 per year.
It cost 30 billion dollars less than expected for its subsidies. The huge drop in per price enrollee eliminates the 3 million less enrolled(than projected) as a being a major factor in that cost reduction. Which means that as the program grows, it will cost less than expected overall.
Table 6
Table 6 shows clearly and definitively that an overwhelming majority of uninsured population now has coverage. Success is hard define though, because yes, this is a goal of the ACA, however, it’s still missing a lot of people.
The trouble with a lot of this is that there were no clear “Success” guidelines given to the general public. What a politician says to the people, and how s/he defines a metric are often different. The more flowery language gives a program lots of room to fail or succeed. But as we’ve all seen, it also opens the door for serious slanted criticism, and interpretation. So instead of speculate what the actual goals of the program were, let’s look at the impact.
Warning here be minor economic analysis:
There are two million less uninsured than projected, and one million more enrollees did not use subsidies. These factors helped keep the percentages about the same as projected. As the number of people who are insured rise, it’s going to affect what those without it are paying nationwide. By using healthcare insurance, their rates are already bargained and while they are the patient they’re not entirely the consumer at the hospital.
e.g. If a thousand people pay rates, each one of them has a voice. Two hundred of them band together to bargain collectively under the name of insurance. Collective bargaining allows groups within that thousand people to command better rates by demanding a certain price. Because the hospital wants a guarantee that it can get those two hundred people lower rates can be negotiated. This in turn can push prices higher for everyone else. When the bargaining groups make up a good chunk of the market it can help push costs even higher. Especially since, the bargaining groups are usually stuck with an exclusivity deal with that hospital.
As more groups arrive and become more of the market, those who aren’t in the groups can face significantly higher rates than they used to. Eventually there is a point at which the groups will command the market together, at this time they will be able to break exclusivity either the group will seek more hospitals to grow its membership and/or because the hospital will try to compete with other hospitals. There’s not really a set point where this can happen, the number of competing hospitals, and area employers can play a large factor in the use and availability of buyers respectively.
The impact of the exchange will allow for more insurers to create more diverse products. It has and will continue to compete among pools of people who before were part of bargaining groups (usually through an employer) or simply individuals who didn’t have access to the insurance(be their rationale to go without: financial motivation, lack of knowledge or what have you).
What the ACA/Obamacare has created is a marketplace for competition, and as the percentage of insured Americans increases so will the prices for those without it, which will encourage them to be part of it.
Referring back to table 6, there is one area where the ACA/Obamacare is assuredly a success. It’s price per enrollee is much less than expected. Keep in mind that the projections for the uninsured population being 2 million less does factor into that, but it’s not enough to cause a drop that large.
The ACA/Obamacare has helped millions of people have access to healthcare, and it’s not as expensive as it was projected. In terms of efficacy and impact this isn’t government cheese, it’s a marketplace where you can afford to choose a health insurance program.























{kind=link}