As someone who got #HepC via Vertical transmission, I don’t just have a lot of thoughts on the matter, I tend to make a lot of comments, public ones. The CDC’s new expansion incorporates almost all of the concerns I’ve voiced to the CDC, CDPH and others over the years when they solicit input from the community.
The latest MMWR from the CDC goes into The escalating prevalence of Hepatitis C Virus (HCV) infections, particularly among reproductive-aged and pregnant populations, underscores a burgeoning health challenge. The Centers for Disease Control and Prevention (CDC) revamped its guidelines in 2020 to encompass universal screening for adults and pregnant individuals, aiming to adeptly manage and curb the proliferation of this ailment.
Epidemiological Trends:
The surge in HCV infections since 2010 is alarming, with acute cases notably tripling among individuals aged 20-39. This uptick correlates with an increase in injection drug use, necessitating targeted interventions. The domino effect of escalating acute infections to chronic conditions emphasizes the urgency for early detection and management. (There’s likely to be a systems issue here, based on a lack of accessible mental health management options, and likely increases in self-medication, among a myriad of other co-occurring circumstances and conditions)
Transmission Dynamics:
Percutaneous exposure to infected blood, predominantly through injection drug use, is a significant transmission route. Perinatal transmission is another vector of concern, thus necessitating prudent strategies to mitigate HCV spread from mother to infant. Understanding these transmission dynamics is pivotal for devising effective preventive frameworks. But its important not to judge people, based on data, rather its imperative we support the person through their diagnosis to cure, as it helps reduce stigma and potential resulting trauma.
Testing, Diagnosis and why this change is important:
The CDC’s 2020 guidelines update underscored universal screening to foster early detection and management. The guidelines propose refined testing protocols for infants and children born to HCV-infected mothers, mirroring the advancements in HCV testing methodologies. This was made possible in part due to public comments from fantastic folks like yourself!
Clinical Progression of Perinatally Acquired HCV Infection:
The variance in clinical progression among perinatally infected children underscores the need for timely interventions. While some achieve spontaneous clearance, others advance to chronic infections, necessitating vigilant monitoring and management to avert severe liver disease. (That’s me, they’re talkin’ bout me ya’ll, End Stage Liver Disease by age 22)
The recent CDC guidelines expand on the diagnostic procedures for HCV infection in pregnant individuals and perinatally infected children. The shift from risk-based to universal screening for HCV during pregnancy aims to bridge the previous under-diagnosis gap. A notable uptick in HCV screening during pregnancy has been witnessed, and all professional societies now advocate for testing perinatally exposed infants for HCV, albeit with variations in the timing.
Clinical Management and Treatment of Perinatal HCV Infection highlights a 6%-7% transmission rate of HCV among perinatally exposed children, (this is almost twice as high as when I was diagnosed with HepC in 1999) with Direct-Acting Antiviral (DAA) therapy emerging as a viable treatment avenue for children aged ≥3 years. The CDC, along with other professional bodies like AASLD-IDSA and NASPGHAN, is steering towards maximizing early diagnosis and linkage to care through perinatal testing for HCV.
Great, but What are the CDC’s new testing recommendations for Hepatitis C Testing Among Perinatally Exposed Infants and Children?
Perinatally exposed infants should receive a NAT for HCV RNA at age 2–6 months to identify children in whom chronic HCV infection might develop if not treated. (Importantly it skips the Antibody test, because the test could indicate a false positive, capturing the maternal antibodies, TBH the antibody test, while a useful epidemiological tool, does beg the question as it to its usefulness for children at all, when, at least anecdotally, it causes a lot of confusion for patients.)
-Infants with detectable HCV RNA should be managed in consultation with a health care provider with expertise in pediatric hepatitis C management.
-Infants with an undetectable HCV RNA result do not require further follow-up unless clinically warranted.
-Infants and children aged 7–17 months who are perinatally exposed to HCV and have not previously been tested should receive a NAT for HCV RNA.
-Children aged ≥18 months who are perinatally exposed to HCV and have not previously been tested should receive an anti-HCV test with reflex to NAT for HCV RNA (Figure 4). (This is an interesting update because it helps with follow-up and appropriate diagnosis, it also shores up holes in terms of late diagnosis, like in my case, where my mom was diagnosed when I was 12, albeit because of my positive case. Although if someone has a negative NAT HCV RNA result, it would seem unnecessary to do an antibody test, which again, just reiterating the likely waste of time and resources of an antibody test.)
Figure 4 from CDC MMWR Recommendations and Reports / November 3, 2023
Cost-Effectiveness Considerations, The CDC conducted a novel analysis to evaluate the cost-effectiveness of perinatal Hepatitis C Virus (HCV) testing strategies, comparing the current method of testing at 18 months to a proposed strategy of testing at 2-6 months. The mathematical modeling study revealed that earlier testing yielded increased diagnoses, improved health outcomes, and was cost-saving at a population level, with savings of $469,671 per year. Universal screening strategies, although enhancing diagnoses and health outcomes, were found to be less cost-effective. The study, evaluated for quality via the CHEERS checklist, substantiated that testing known exposed infants at 2-6 months is both cost-effective and beneficial for better health outcomes.
Hepatitis C Elimination
Ongoing monitoring and potentially revising recommendations in line with evolving epidemiology and treatment modalities for hepatitis C during pregnancy and among children are on the CDC’s radar. The quest for more data on universal screening, prevalence rates among pregnant persons, and the natural history of perinatal hepatitis C is unending. The deployment of highly sensitive and specific NATs for RNA detection among perinatally exposed infants and children is a beacon of hope in identifying those with HCV infection. This initiative aligns with the broader agenda of national hepatitis C elimination goals, showcasing a concerted effort to ensure no population is left behind in this health crusade. The road towards hepatitis C elimination is laden with challenges, yet with cohesive strategies and relentless pursuit of early diagnosis and treatment, strides towards a healthier tomorrow are within grasp. As someone who understands the impact of a pediatric diagnosis of Hepatitis C, in terms of the emotional experience, and challenge with family interactions and stigma, this is a welcome update to capture potential cases that might otherwise be missed.
Get Tested, Get Treatment, Let’s End Hep C!
Panagiotakopoulos L, Sandul AL, et al. CDC Recommendations for Hepatitis C Testing Among Perinatally Exposed Infants and Children — United States, 2023. MMWR Recomm Rep 2023;72(No. RR-4):1–19. DOI: http://dx.doi.org/10.15585/mmwr.rr7204a1
Well, this was supposed to be about the economy, but that’ll come later. While each of these *can* be read independently, it’s best when read together: First Article, and Second Article.
First, let’s talk about the title of the article, “Trust me, it’s raining.” We’re diving into the importance of public trust in agencies and how, unfortunately, science isn’t always the driver of a decision as much as we’d like to think it is. Because in May, the C.D.C. and the Biden Administration’s messaging was akin to pissing on our shoes and telling us it was raining. Unfortunately for us, when it rains, it pours.
It’s also meant as an analogy we’ll talk about later when it comes to preparing the tools in your intervention toolbox, how they layer, and how to think about daily covid protection, more like weather, or well, rain.
A few weeks ago, amid the new mask rules, the C.D.C. also acknowledged that transmission has been occurring among the vaccinated population. For some reason, this tidbit seems to be very misleading among folks, from advancing concerns about the effectiveness of the vaccine vs. the new fears of Delta/V.O.C.s… but this reality makes their previous guidance seem suspect.
Because in terms of the data and Literature at the time, it was. It was a political decision to not simply repeal the mask guidance prematurely, but to encourage abandonment of interventions once vaccinated… Public Health experts have been beside themselves this entire time. When vaccination rates scuttled, the hope that F.O.M.O. would encourage folks to get vaccinated not only fell flat but helped encourage cases to spread.
In my previous articles, I’ve explained the reality reservoirs play when large groups of folks refuse to abide by interventions designed to decrease the incidence of COVID19. Those being mask-wearing, physical distancing, increased hygiene/handwashing, and of course vaccination when medically reasonable.
Before we dive into why the new C.D.C. guidance makes sense and how we should incorporate the new “covid weather map” into our daily lives, let’s talk about that last intervention.
The vaccines are solid, they work well,and are unlikely to require a booster any time soon. In November/December, that may change. (although the WHO, taking a political knee and saying please stall until September for boosters to the developed countries pushing boosters)It’s important that the target for vaccination should be the most folks getting fully vaccinated before boosters become common in developed countries, if we want to eliminate the global recurrence of new VOCS at the rapid pace we’ve seen. “In the context of ongoing global vaccine supply constraints, administration of booster doses will exacerbate inequities by driving up demand and consuming scarce supply while priority populations in some countries, or subnational settings, have not yet received a primary vaccination series. The focus for the time being remains on increasing global vaccination coverage with the primary series (either one or two doses for current EUL vaccines).” as stated by the W.H.O.
That being said, if our current V.O.C. trend continues, sometime next year, a booster would likely help the more vulnerable populations and may be indicated for everyone should the virus find new footholds. The science behind boosters is sound, and the data reflects the protective quality of the vaccine. We have always known that the vaccine likely protects to a certain degree against infection but that it does not always prevent transmission.
All my pencils just say Drugs now
Our current messaging on the pandemic is, well… bad. It’s exclusive, shame-inducing, and it’s basically the same strategy we always use: shame, aka peer pressure. Does it work? To a degree, but it has a weak range of effectiveness, it always has; Project D.A.R.E. is ineffective(West, 2004). If you suspect it works, I D.A.R.E. you to consider other similar strategies met with bucking shame and tribalism like the “War on Drugs” and, well, Condom use.
When we hear messaging on vaccination, it blames the unvaxxed for all the problems we’re experiencing, as if they are the source of the new problems. Which while partially accurate regarding V.O.C.s, it’s also important to remember that this is a virus. And no one is at fault here.
Leaders who use their platform to spread misinformation or disincentivize folks from taking the vaccine or following other interventions do bear a degree of blame for which society should interpret sooner rather than later.
It’s important to consider the US CDC messaging isn’t happening in a vacuum, it’s happening in a world where 20-30% of the population cannot afford the vaccine under the current conditions, and somewhere around 20% are struggling to access for a lot of different reasons, but mostly to do with cost or the convenient opportunity to commit genocide with less potential blame. Currently, about 30.4% of the world is at least partially vaccinated, only 15.8 are fully vaccinated, and the U.S. just passed the 50% mark on fully vaccinated (two weeks after the last jab.) Pandemic is global, an important reminder here is that V.O.C.s have come from other countries, as well as being amplified in the U.S. Importation of cases will constantly be an issue when states like Florida are a hot-bed for the circumstance due likely in part to DeSantis political ambitions overweighing safety for the American people. Between instituting a mask-less requirement for all Florida schools and threatening district leadership with pay cuts if they try anything(and now that pushback), I don’t think we’ve yet seen the worst of his policies, as they continue to ignore evidence and enjoy cherry-picking data.
The U.S. C.D.C. messaging creates a specific narrative that does not help to eliminate the pandemic.
The current C.D.C. messaging focuses on pressuring the unvaccinated as the cause of V.O.C.S. and the reason for our current surges, which is a half-truth. The vaccinated, are, unfortunately, also spreading SARS-CoV-2, as much, if not MORE, than unvaccinated due to their larger numbers and similar lack of adherence to interventions; the difference is in how far that spread goes. The evidence regarding vaccinated folks carrying the virus has been known for some time; the initial SARS-CoV-2 virus had been shown to be transmissible among vaccinated, but far less than typical. We also suspected V.O.C.S. might change the game up. On March 10th, J.A.M.A. Viewpoint from the C.D.C. “A growing body of evidence suggests that fully vaccinated people are less likely to have asymptomatic infection and potentially less likely to transmit SARS-CoV-2 to others. However, further investigation is ongoing.” (Christie, 2021)
“The risks of SARS-CoV-2 infection in fully vaccinated people cannot be completely eliminated as long as there is continued community transmission of the virus. Vaccinated people could potentially still get COVID-19 and spread it to others. However, the benefits of relaxing some measures, such as quarantine requirements, and reducing social isolation may outweigh the residual risk of fully vaccinated people becoming ill with COVID-19 or transmitting the virus to others.” (Christie, 2021)
This is from a paper the C.D.C. director co-authored; the tone was already being set for the shift in messaging; however, what’s certain, was that we should not discourage interventions but relax measures according to regional outbreaks. California’s tier system successfully allowed counties to better control their circumstances; the lessons learned would have been easily translated, as they more recently have been in the new C.D.C. guidance.
But…following the strange shift to ENCOURAGING vaccinated folks to resume all activities without consideration for interventions was at the very least reckless. The medical blog site The Conversation echoed how most Public Health folks felt about this strange messaging. “Vaccines can be great at preventing you from getting sick, while at the same time not necessarily stopping you from getting infected or spreading the germ.” (Mishra, 2021)
We knew caution was essential to maintain because many suspected immune escape and viruses to continue to create potentially new V.O.C.s when the subvariants affect one another. We knew immune escape was a potential problem, we suspected increased transmissibility of new V.O.C.s, and yet not until weeks after Biden’s celebration regarding successfully not reaching 70% by July 4th and more information coming out about Delta did the messaging shift.
For those of you who are interested in high-value content regarding accurate information about COVID-19, might I suggest https://www.covidhealth.com/ and https://www.unbiasedscipod.com/ They put out lots of well-designed graphics and sharables like the one below.
from Unbiased Science Podcast
Important regarding the Delta V.O.C., The increased transmissibility is roughly twice as potent as the original strain, increasing viral load early on by as much as a thousand times higher. This not only indicates significantly more pre-symptomatic transmission, but importantly it improves the sensitivity of our PCR tests. Previously, PCR tests had a false negative rate which decreased to near nil close to day 5, but due to the increased viral load, Delta is detectable earlier than the original strain. Overall potentially improving test sensitivity by upwards of 10-15% due to the smaller windows of false negatives.
People were grossly unaware of the reality of the problem partly because the news doesn’t understand public health. Occasionally the NYT has been helpful regarding their data; however, their interpretations, opinions, and articles vary immensely based on its author.
This discourse was confusing for the general public because of media trash like this.
Made more confusing by choices like this from the C.D.C.: As explained in my previous article, the C.D.C. isn’t really looking for breakthrough cases, although the states are recording data on their own. Given the political climate, this *seems* not well thought through. It’s also important to note that breakthrough cases are defined by two weeks following vaccination, which puts partially vaccinated folks into the general lump. DEBLASIO, DID YOU READ THAT? Why the Capslock? Because the Mayor of New York City’s strange vaccine I.D. requirements only need one dose to count and may repeat the Springsteen debacle of vaccine nationalism, because what vaccinations count? L.A. reinstituted a mask requirement, which is…well…easier, more inclusive, and pisses off people who don’t want cloth on their face. The LA requirement also has no teeth, so most folks will and have likely ignored it to a degree, which we’ve been seeing alongside growing tourism likely importing cases.
But now the C.D.C. finally is on board with an actual solution, and of course, folks are doubting the agency…again. Do they deserve the doubt? Yeah, I’d say they tarnished the trust with the U.S., now multiple times over masks, so this was an epic fail on the part of the C.D.C. to do this, in this fashion.
But now that we do have reasonable guidance, let’s talk about how we should live with this pandemic.
We’ll get into the nitty-gritty of just why the C.D.C. messaging is so bad after this analogy.
Gritty is a mascot and the logo are owned by The Philadelphia Flyers
IT’S RAINING, MEN.
However you consider the Coronavirus/SARS-CoV-2/COVID-19/’Rona Pandemic, its essential to consider how a public health body should explain preparation for everyday folks.
We should think of SARS-CoV-2 like we do precipitation. Now, with better testing, better maps, integrated map tools into Google Maps, this type of analogy can make a lot more sense.
First, we have to look locally because that’s where the problem lies. A Pandemic in this sense is considered by its millions of regional outbreaks. So we can think of it as a massive Global super-Hurricane capable of producing all weather phenomenon.
Does it sound potentially terrifying? It should. Our toolbox of protection against rain may be raincoats, umbrellas, boots, maybe a towel by the door. For snow, we might need a snow shovel, salt, thicker coats, snow boots, etc.. We prepare for a pandemic in the same fashion, it’s just a little harder for some folks to initially see this because it’s a generally invisible threat.
The prevention toolboxes listed above are for an individual, and there are more for the community, and the State, should the weather become too burdensome on the individual. There are also toolboxes for response, maintenance/long term, and importantly for the future, meta-analysis, but let’s focus on what you can do, and maybe a bit about what some stuff around you can do.
These are the tools in our toolbox for an individual by importance:
1. Getting the Vaccine, in terms of rain( SAR-Cov-2), It’s like having a scotch guard bubble, one’s feet might get wet, and the bubble gets scratched up as it encounters things like hail(V.O.C.s).
2. Wearing a mask is like an umbrella, so if any water does get in, one is still dry to a degree, but one’s feet still get wet. (benefit is an umbrella can reduce the rain for others nearby, but don’t share masks)
3. Interactions are a combination of physical distancing and time. These are the boots, and how they’re used determines what type of boots they are and to what they’re resistant. The less time an interaction requires, the stronger those boots are, the greater the distance the interaction requires, the more protective those boots are. E.G., If an Interaction takes 15 minutes, and someone can keep a distance of 6-8 feet, that interaction previously ran a low risk but now runs a low but higher risk with Delta. It would be like wearing boots with worn soles a small hole in moderate rain; socks likely will get wet the longer the stay, and with random hail(V.O.C.s), it’s making the water splash about getting the bottoms of pants wet.
4. Airflow, often this can be considered Inside Vs. Outside. There are lots of ways to improve or increase airflow, opening windows, using air purifiers, increasing the cubic footage (typically heightening a room), adding negative pressure or exhaust fans. Each of them, like every intervention, mentioned, layers to add protection against SARS-CoV-2 and its V.O.C.S.
5.Hygiene isn’t just washing your hands. In this case, it’s cleaning your hands after you interact with things in new buildings or commonly touched items outside. It’s avoiding touching the face, nose, and eyes while not in the home. It’s the analysis of our washing routines to make sure we enter our homes clean, which can mean taking a shower after a long day at work if work is in a public or shared space with lots of people. Hygiene also reduces our risk of getting multiple illnesses. Some folks might wear lycra gloves to avoid constant handwashing, but they should rotate through sets as they go from location to location.
6. What? There are more tools?! What else can we do? Vote for political candidates who aren’t actively telling others not to or disable their ability to do any of the above. Really. This is by no means an endorsement of any political group; it’s just common-sense Public Health. Leaders who broadcast and elect to enact policy making an outbreak easier are objectively a bad choice during a pandemic.
7. Hah! There’s even another one, because the Internet. Correct misinformation to the best of your ability, even your own. The Scientific Literature is constantly growing and correcting itself, and when agencies interpret this, once an Administration is involved, it has to consider what obligations or national temperament may require. This is part of why C.D.C. Director Walensky removed the mask requirement because it would release tension regarding intervention compliance, giving a break, for what she would have likely suspected, was a wave coming in the Fall. The likely additional guidance by the White House to disregard all interventions once vaccinated was likely weighed with the unknown of Delta. The Literature expanding to include the significantly higher transmissibility put pressure on the C.D.C. to install the current system, one which always should have been the guidance. But Literature doesn’t guide every government decision; there are a lot of data to consider, including compliance with interventions. So government agencies have a degree of fallibility here. But it’s crucial that when we correct misinformation, we shouldn’t be a dick about it, speak honestly, but withhold that new Government Encouraged Outrage.
For a moment, to see how the messaging is doing to improve vaccinations, let’s return to the K.F.F. Vaccine Monitor to see what stalwarts likely remain, besides those of us with chronic conditions who require the timing to figure out when to vaccinate or who simply cannot given the current guidance with their doctor. We should assume that the vast majority of them would likely answer “Wait and See” and a few as “Definitely Not”, but not enough to break 4-5% and 1-2% respectively of the whole. So about 20% of Americans still leaves many folks who aren’t interested in vaccine-induced immunity for whatever reason.
But the most compelling thing from this month’s K.F.F. Vaccine Monitor was this unsurprising comparison “News Of Coronavirus Variants Has Caused Some Adults To Change Behavior, Two In Ten Unvaccinated Adults Say It Has Made The More Likely To Get Vaccinated” vs “A Majority Of Vaccinated Adults Say News About The Possibility Of A Booster For The COVID-19 Vaccine Hasn’t Caused Them To Worry About COVID-19 Protection, Black And Hispanic Adults Slightly More Concerned.”
These data illuminate that the white house messaging DARING folks to get vaccinated to avoid creating V.O.C.S. and blaming them for the new surges aren’t having the desired effect of increasing demand for vaccination.
So it’s time to consider what’s next. The increased vaccine employer requirements are absolutely squeezing the “only if required” crowd down to zero. Still, the remaining potentially 15% by the end of this year who will be Choice Unvaccinated might be enough to continue this nonsense for another year yet, instead of going from mitigation to control like in New Zealand or Taiwan.
How do we convince the stalwarts? Talking to them helps, but only when it’s productive and informed.
A big thing, though, is honestly, ignore the big fluffing. The thought-leaders encouraging anti-vax thrive on being the underdog and defending their position, don’t give them clicks, just brush it off like the nonsense it is, and also don’t feed the hating on them, ya know, like the U.S. C.D.C. messaging inadvertently does.
It’s important that we all agree on something here, though, that no one deserves COVID-19. Leaders do bear some responsibility; however, that doesn’t mean someone deserves a life-threatening condition that could result in a chronic illness or death. If we want to get through this pandemic, the only way we can is together.
By considering the Interventions relative to the danger around us, much like we do with weather every day, we can best take caution to protect ourselves and our communities. We may not always need to wear a mask all the time, but when the risk is high, we should take as many precautions as possible and use as many tools as we can carry.
Get Vaccinated when/if you can. Wear a Mask indoors, in crowds, and in mass transit. Also, consider the other tools as the situation demands.
References
Christie A, Mbaeyi SA, Walensky RP. C.D.C. Interim Recommendations for Fully Vaccinated People: An Important First Step. J.A.M.A. 2021;325(15):1501–1502. doi:10.1001/jama.2021.4367
Lazarevic I, Pravica V, Miljanovic D, Cupic M. Immune Evasion of SARS-CoV-2 Emerging Variants: What Have We Learnt So Far? Viruses. 2021; 13(7):1192. https://doi.org/10.3390/v13071192
Levine-Tiefenbrun, M., Yelin, I., Katz, R. et al. Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine. Nat Med27, 790–792 (2021). https://doi.org/10.1038/s41591-021-01316-7
West, S. L., & O’Neal, K. K. (2004). Project D.A.R.E. outcome effectiveness revisited. American journal of public health, 94(6), 1027–1029. https://doi.org/10.2105/ajph.94.6.1027
If you’re reading this first, check out my initial article in our COVID-19 series. This is the second article in the series. I’m an Infectious Disease researcher and MPH working with ending epidemics. I also happen to work in Workforce Development/Life Sciences and have a background in Economics, PoliSci, History, Law, Policy, Healthcare, Counseling, Advocacy, and Marketing.
As a patient advocate for over ten years now, when I look back at the majority of my moments as a patient, I look back at my powerlessness. For the vast majority of patients, powerlessness is an overwhelming reality when it takes hold. It can be from the initial diagnosis. It can be when certain symptoms begin or often when they find out that there are no treatments, even on the horizon. In my case, I was lucky that treatments were developed in my lifetime to cure my of my lifelong battle with Hepatitis C. But those fears, that impotence, is very real and very common, at least for some time in many patients.
Norovirus is relatively harmless for most folks with healthy immune systems. Still, for the elderly or folks with hampered immune systems, it can be a significant challenge. In rare instances, death can occur. On cruise ships over the past decades, Noroviruses have become so common that most cruise ships have enhanced safety requirements to protect passengers and staff. The CDC has managed these cases and provided guidance in this arena for as long. The CDC does this through the Vessel Sanitation Program, since 1975 when it was created. The CDC indicates its specific jurisdiction of cruise ships carrying more than 13 passengers and a foreign itinerary in US ports.
WAIT, I THOUGHT THIS ARTICLE WAS GONNA BE ABOUT COVID AND MASKS AND VACCINE IMMUNITY.
It is, and it isn’t; it’s also about the legal stuff and vaccine “passports” as well as a spiritual continuation of When Captors Masquerade as Allies. Let’s talk about the state, which will likely be a consistent reservoir for COVID-19 and new Variants Of Concern, Florida. And has led the country in growing VOCs, having the highest amount of VOCs in April prior to the new COVID-19 dashboard, and currently as of July 2 , maintains 2,381 over the two week period, vs. 2,598 in CA, a state with twice its population and equally a destination state for tourism. Florida in April had double the cases of any other State among VOCs, and that trend seems to be continuing with DeSantis’ policies standing in ignorant defiance of how infectious disease works.
So the CDC’s VSP has always been the only one with jurisdiction here. Cruise ships have a very specific carve-out due to the health hazards historically associated with Cruise ships. So why do I care about Cruise ships? I don’t really; my personal experiences leave much to be desired, but this situation in Florida is problematic at best, because it can easily lead to higher importation of cases when not monitored properly.
DeSantis is arguing on one hand that the CDC’s sailing limits restrict Florida’s revenues while claiming that vaccine prevalence is so widespread, so much so, he’s willing to punish the industry he’s claiming to protect. What’s even weirder here, both cruise ship passengers and companies seem pretty happy with the enhanced protections, something DeSantis doesn’t seem to be considering in his stand against reasonable and basic public health measures.
As we consider these interactions on a national level and see how inconsistent actions among people with authority wielding these clubs against one another. Where a disagreement between federal marshalls who refuse to disclose vaccination status meets a judge who demands to see it while refusing masks in his courtroom. This interaction showcases the challenges when political intention creeps into our bureaucracy; both parties seem to be acting on partial information. The Judge, being in a public court, should hold that all people inside are wearing masks when vaccination status is unknown, while the Marshalls should have known to comply with the court, providing the documentation. The CDC and Circuit courts generally agree on the following:
In courtrooms, if only vaccinated people are in the courtroom, masks will not be required. If anyone is unvaccinated or the vaccination status is unknown, masks will be required unless the presiding Judge permits otherwise.
But it gets very tricky when the CDC stops holding the bar up for the country regarding actions for public health safety. State courts, even county courts (this site lists them all out), all have different rules regarding vaccination, status, and masks during the pandemic.
One central theme, though during all of this pandemic, has been folks blatantly defying public health orders for a surprising number of reasons. Reasons varying from political free speech, their freedom to breathe, believing it’s worse for your health, believing they don’t work, to just not wanting to.
These actions bear responsibility for facilitating the spread of the virus. As a person who lived with Hep C nearly all my life, I was constantly aware of the very real potential jail time which could come into play if I intentionally hid my positive status with a sexual partner even though Hep C isnt’ an STD, and they were to be infected. These rules regarding STDs disproportionately affected the LGBTQ community, and thankfully these laws are being revisited. So there are circumstances where we can see exceptions, like for folks who are vulnerable and could not wear a mask. But here, what we’re seeing is closer to intentionally infecting others, the goals of anti-maskers are wide, but some do want to naturally create herd immunity(which would make more VOCS just like Manaus), in spite of how little we know. (side note the Unbiased Science folks helped this one, it’s a solid article.)
The trouble again comes before with anti-maskers, and soon with the maskueraders, their actions likely add not only to further spread of the virus but also strain community relationships and introduce stress and tension into environments.
Actions like these are willful defiance of a uniform strategy for public health, something essential for any public health strategy: unity. To encourage maskueraders by pardoning their crimes of willful defiance of public health orders during a national emergency, his actions also discourage trust in the CDC and public health institutions.
The importance of patience is essential to our survival as a nation.
There is a considerable race to vaccinate and protect as many people as possible, as new variants of concern pop up, which have increased transmissibility or immune escape. On a global scale considering India and Australia’s recent surges, our premature revelry in the US will likely lead to unnecessary deaths. Thankfully Australia has mechanisms acting in unity which may help them considerably in containing Sars-CoV-2 in Australia. But importantly, from the Australia case, just as in many circumstances in the US, the overwhelming majority of cases occur among unvaccinated individuals and are increasingly VOCs
Image of viruses from DW
As the Delta variant displaces its progenitor rapidly, more and more public health officials are encouraging mask use, including the WHO, Los Angeles and more recently, Sacramento. Folks who are immunized should likely wear a mask indoors, in crowds, or in mass transit for the duration of the pandemic.
VOCs like Delta and Delta Plus throw a big wrench in the reality of data being presented. In the US, an overwhelming majority, almost 99% of severe cases, occur in folks who have yet to get vaccinated. So let’s focus on those who are vaccinated but test positive for covid-19, Breakthrough infections/cases as they’re called.
An important consideration: Breakthrough Infections, bottom line, does everyone need a test?
Breakthrough Infections are complicated, and while early on, the majority were asymptomatic, about 10% of the 10,262 breakthrough cases as of April 30,2021, were hospitalized, and 2%(160) died. The median age being 82, indicates that in the rare cases of breakthrough infection, death trends skewed towards older; perhaps importantly, 64% of hospitalized cases were VOCs. It’s also important to note that there are likely significantly more asymptomatic cases of COVID-19 among the vaccinated population. However, their infection may never be noticed or included in data, due in part to the lack of priority on testing among vaccinated individuals at this time. Deprioritizing testing among a population can cause testing bias in the system, which may impact the data.
Without the CDC holding the bar on what mask and vaccine standards we should maintain, we end up with more chaos than needed during a very wild economic time. A hospital in Texas is fighting for its ability to ensure that its employees are vaccinated, facing a lawsuit from 117 employees who did not want to get the vaccine. Cases like this will come about across the country; however, there is no standing, so it is unlikely many will succeed. Without proper guidance from the CDC as to best practices, at the very least, states all have incredibly different policies, which will likely only further expand reservoirs, as mentioned in my previous article. Reservoirs naturally encourage new VOCS if they have a high enough population of unvaccinated folks. It’s also important to know that now the Delta variant accounts for the majority of new infected cases. All the more reason to get vaccinated to reduce the potential for VOCs.
Here’s something which may or may surprise you: I’m not for vaccine passports, but I’m also not necessarily opposed to them, as they don’t actually impede on privacy or health status information.
California is attempting something similar, but still uniquely Californian, in that, it only applies to places you have to pay for. Conceptually, it limits the ID requirement to systems that need to know the information due to increased risk and a cost barrier, and who knows when it will actually be instituted, or how it may yet change.
Different but related, just on more economic, legal matters regarding COVID-19, more lawsuits are going forward against governments for loss of revenue. A reasonable consideration for small and medium-sized businesses who suffer(ed) or discontinued during the pandemic. We’ll take a deeper dive into the economics of all of this in the next article: When the Economic Flywheel Isn’t Flying.
These solutions to vaccine status awareness may prove helpful in time if there is social acceptance. But again, this harkens back to an earlier message: unity. Public Health efforts, when not unified, fluster and have significant holes. Public health efforts require immense trust, buy-in, and consideration from each community involved. Without all of walking the same route of protection, it weakens any potential defense. So, however, we move forward with vaccination identification, we should hope and encourage equitable solutions.
Unfortunately, a pandemic affects the world, which also means that as VOCs spread around the world, we are gravely affected by each other misdeeds, misconceptions, or misunderstandings regarding COVID-19. It also means that vaccination efforts be universal across the globe to ensure the eradication of the threat of COVID-19, much as we’ve done for Smallpox and Polio, rather than as we’ve done for Malaria, HIV or Viral Hepatitis, which run rampant around the world, killing millions each year while the US has significantly reduced death counts comparatively. Smallpox and Polio had global vaccination efforts with few restrictions on patents, while HIV and Viral Hepatitis face patent restrictions (which create temporary monopolistic pricing for the patent holders), among dozens of other potential barriers. There are a handful of efforts to like COVAX and #FreeTheVaccine, which are trying different ways to encourage the sharing of the vaccine to rid the world of this problem.
It’s important to remember that Polio was solved here in the US so quickly because of the refusal of Dr. Jonas Salk to patent the Polio Vaccine. In his famous words: “Could you patent the Sun?” A comment not only inspires parable but an essential legal reference to the reality of products of nature. Obviously, when a product like mRNA comes into play, it’s a lot more removed than a more typical product of nature, so the logic here is more complicated. Here, we look at the result required for global stability: universal vaccine availability and seek to understand solutions to that complex problem. While the United States has held that patents in this specific circumstance would benefit from flexibility, Germany, has strictly opposed such patent sharing. Mind you, in the US, multinational pharma companies are still fighting this stance. So it’s unlikely that patent sharing, waiving, or other exceptions will pass without obstacles.
Another organization is attempting a different strategy; the Global Immunization Action Network Team (GIANT) is a global resolve to improve global public health outcomes by combating vaccine hesitancy through effective, sensitive, science-based communication and education. Vaccine Hesitancy is a complicated demon to face. The other side of vaccine availability and equitable access is the desire to understand vaccination’s safety benefits. GIANT isn’t focused on COVID-19 specifically, but it encompasses it; but for those like myself working with End The Epidemics and No Hep 2030, among other elimination initiatives, comorbidity is a big target we’re focusing on. Comorbidity is having multiple infectious diseases or conditions. Comorbidity just amplifies the problem at hand, whatever the condition. COVID-19, being so widespread, has complicated life for folks with chronic conditions looking to avoid additional comorbidity because that could mean death. So GIANT’s approach towards messaging and education are critical while figuring out how to make the vaccine more accessible.
Okay, again, this is terrible! Infighting, and confusion, lawsuits galore! What can anyone do?
If you can, get vaccinated, Me, getting vaccinated July 5th.
As a transplant recipient , I’ve been eligible for the vaccine in CA, since February. But in the heat of my MPH, learning my chair had an adverse reaction to the vaccine reminded me of the importance of timing. Timing for side effects is something folks with chronic conditions have to figure out with treatments, vaccines, and other health procedures. I’ve personally had to plan 6 Hep C Treatments, thankfully. The new ones aren’t so bad as far as side effects, But the old pegylated interferon and Ribavirin are an awful experience. Months of exhaustion, mood swings, skin issues, and significant blood loss were important to time these in my life. I injected on Fridays to have the weekend to take the brunt of each interferon injection, which felt like the nights of a thousand flus. Between my MPH Thesis, new caretaking needs for a family member, some personal health concerns, and other serious projects, I wanted to make sure that if the vaccine had any serious side effects, that it would be on my time, that it wouldn’t be too much of an additional burden.
I also was watching several studies on liver transplant patients to see if the outcomes were different. (As a transplant recipient, according to a recent study, mortality is about 20% with COVID-19, but with the vaccine currently, there have been no reported deaths due to COVID-19 among transplant recipients, so although we don’t know how well the vaccine confers immunity in transplant patients due to their immunosuppression, we can tell the outcomes.) Importantly, I also note that I don’t have any allergies, so I knew I could pop over to Vons and take it. If I had more common allergies, I personally would have taken it at a clinic, JIC. So I arrived at yesterday, at a local Vons. For those who can vaccinate, please do, and encourage folks around you to do so as well. Important note: There are hundreds of thousands of folks in my situation who planned when and how to vaccinate because for us, it’s not as simple as walking in. There are plenty of folks with chronic conditions who decided, “you know what, I’m just going to go for it,” and we appreciate their choice to lead us through the crisis. But the choice of when to vaccinate can be complicated. So it’s essential when we talk about vaccination with our close friends and family that we also keep this in mind. It’s also important to remember that among all the revelry, this pandemic isn’t over.
FF Meme about family and getting vaccinated
Honestly, if you are not in a position of power to be able to help folks, improve messaging, finance, research, or otherwise seal holes in our global vaccine response. Then there is not a whole heck of a lot you can do, but… there is still something pretty big.
First, you can get the vaccine if it’s available and you are physically able to tolerate it. Regardless of vaccination status, wearing a mask indoors, in groups, and in mass transit helps decrease spread and thus the potential for VOCs. For folks who are still unvaccinated, wearing a mask, maintaining six feet of physical distance, preferring outside interactions, and reducing interaction time, can be helpful.
If you still want to do more, you can. Talk with your friends and family, make sure everyone who can vaccinate is vaccinated. Chat about how important mask use still is while indoors, in groups, or in mass transit.
Important note: as vaccination rates rise and cases decline, it’s also essential to consider the positivity percentage of COVID-19 regionally. The lower the number of cases and positivity percentage on a regional dashboard, the safer it can be without interventions for those who are vaccinated; however, it is critical to consider your own personal health circumstances. If there is no dashboard available, then, much like the court case mentioned previously, the best practice would be to wear masks.
We haven’t even talked about Long COVID, the chronic condition resulting from COVID-19. A condition that plagues asymptomatic and severely symptomatic alike, nor its impact on our public health system, but we’ll get there next time, in the next article: When the Economic Flywheel Isn’t Flying.
This series will take as long as needed.
Read it for as long as you can/would like; I appreciate your ears/eyes and hope to also hear/read your considerations.
As of June, 2021, I will have been eligible to get the COVID-19 vaccine for over four months now as a Solid Organ Transplant Recipient. I am a person who received a liver transplant, younger than the average at the age of 35. My transplant journey is a rough story concerning my life-long battle with Hepatitis C, six treatments, and six plus years in End-Stage-Liver Disease you can read more about the story here.
Because this story isn’t about me, per se, but about the circumstance that I find myself in, along with so many of my peers. Before I explain further all of this, some background is in order as to explain the importance of understand the nuanced differences in vaccine hesitancy and folks who are among the “unvaccinated”.
I belong to part of a large group of vulnerable folks, collectively, spoonies is the best term here. Because the complex mix of auto-immune, genetic, medically induced and viral infection induced immune responses include lots of folks. From folks with certain cancers, folks with HIV, to folks like myself who take medication which suppresses our immune system.
Collectively it’s estimated that we comprise about 4-7% of the United States population, with about 2.7% of the population being transplant recipients like myself.
Many of us who might benefit less from the vaccine, will continue living as if nothing has changed. Masking regularly indoors, outdoors in groups, increasing our hand-washing and keeping some physical distance from others, especially if near crowds, and minimizing interactions.
There are many estimations of when Community Immunity may take hold, somewhere between 70-90% is the average of all the literature and articles I’ve come across. In Brazil, the efforts to induce natural herd immunity, in part by relaxing non-pharmaceutical interventions like mask wearing, resulted in the population of Manaus having as many as 76% of the population infected, and also provided us with the P.1 Brazilian variant now being referred to as the Gamma variant. So to be at the the functional level needs to rely more heavily on vaccine induced immunity, in part because it potentially lasts longer. More importantly it is more robust than natural immunity as more documented cases of reinfection have occurred through natural immunity, especially in regards to Variants of Concern. And it slows the potential for new variants due to significantly reduced levels of viral procreation when vaccinated. (aka less viral load in vaccinated folks means less potential for evolution into new variants, because it doesn’t generally evolve in the wild, just in people/animals.)
As Variants of Concern continue to appear due to the uncontrolled and widespread state the pandemic is currently in, we must consider that these will eventually impact transmissibility of SARS-CoV-2., as both the Alpha variant (AKA UK variant AKA B.1.1.7 variant) and the Beta(AKA South African Variant AKA B.1.351 Variant) have. How this in turn is met with growing vaccine uptake, time is slowly revealing.
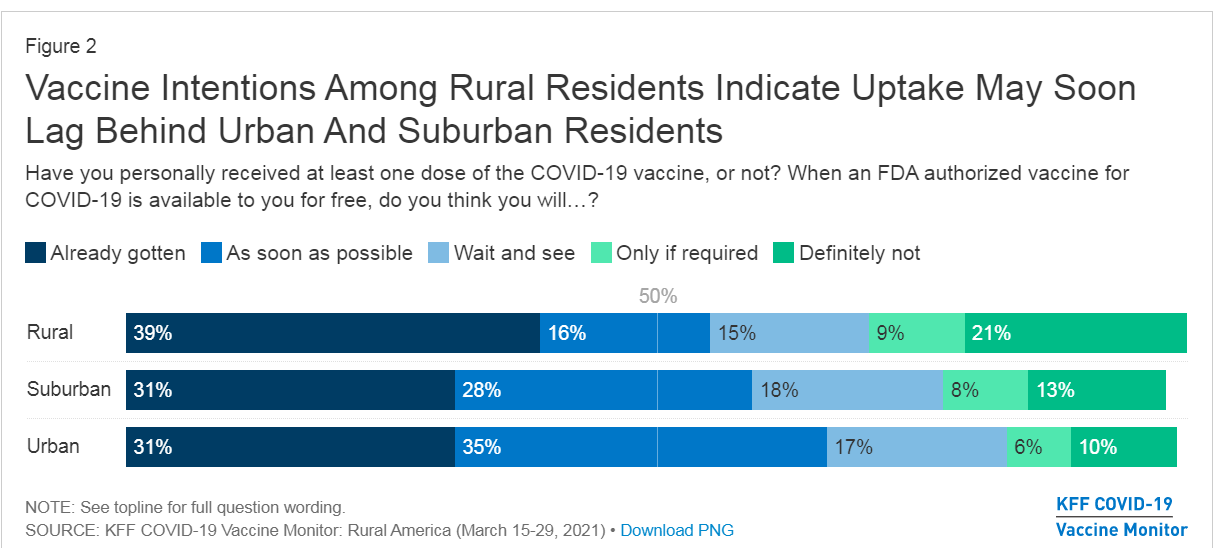
For those not familiar, this is the Kaiser Family Foundation Vaccine Montior. An important constant pulse on vaccine uptake and trends here in the United States. Crucially, it has been monitoring the Already got it vs ASAP vs Wait and See vs only if required vs Definitely not.
Within the Spoonie communities some of us may attempt to get the vaccine, anecdotally, many who have reported higher than average instances of side effects, or no effect whatsoever. For others in the Solid Organ Transplant situation concerned about the vaccine check this out, it won’t help you make your decision, but it might help inform it a bit more, especially if you check their references.
Now for the reference to the title of this piece, who are these captors? The vaccine hesitant for non-medical reasons, and most importantly those who would refuse themselves and their children the safety of a protective vaccine.
For spoonies like myself who long for a return to seeing friends and family, going to a graduation, a wedding, even a funeral, there is little hope in reaching community immunity without the help of those who also fall into haven’t gotten the vaccine category. For veterans of the spoonie community, we’re no strangers to phonies, con-artists, scammers, and conspiracies, especially on the internet, not to mention the people who call them out, and people who accidentally call out real Spoonies. When you achieve a certain level of fame on Instagram, some spoonies find themselves fighting off fake accounts, copies of their own who grift unexpecting folks. We’re used to folks pretending to be disabled standing next to us in line for a Disability Access Pass in Disneyland, or folks who claim medical exemptions for hardships where none exist. And we’re used to the increased scrutiny and disbelief of our condition if not visibly apparent. For some it reinforces imposter syndrome, it encourages them to avoid seeking help, there are layers to these problems which are important to know exist as we explore the reality for folks like me in 2021 in regards to vaccine hesitancy.
The alarmingly high number of 13-15% of folks answering definitely not to the vaccine likely includes a small portion of folks like myself to more extreme cases who absolutely cannot get any COVID-19 Vaccine. But even without considering that, we can be assured that this % is not consistent state-by-state, and significantly different between rural and urban populations.
We see that among rural populations, the majority of folks who would not be vaccinated number as high as 21% on average. It is impossible to extract from this data where spoonies might fall. Because some of us have already gotten the vaccine, many like myself wait and see, and some already know they cannot take the vaccine, or are so alarmed by side effects they’ll only do so if required, and even then they may quit or be fired.
Let’s assume the upper limit of 28%, a stat where every spoonie cannot vaccinate, with a lower limit of 23%, where only a few spoonies vaccinate successfully against SARS-CoV-2. It means that on average among rural populations the vaccination rate might not breach 72-77%, clearly around or below the 76% which existed in Manaus for their attempt to gain Herd Immunity. Again, Vaccine Induced immunity is likely stronger against SARS-CoV-2 and its VOCs, but at such low rates of vaccination, it poses a significant danger in a different way: Reservoirs. Reservoirs (of infection) are individuals, animals, plants, substance, soil or a location which the virus lives and multiplies. Reservoirs make it hard to eliminate an epidemic, in the U.S. and other countries the prison system does this with Tuberculosisand Hep C. As populations in the prisons have significantly higher incidence of disease than populations outside prisons. Reservoirs don’t’ work well if those folks aren’t intermingling but unfortunately…
Another chart form KFF tells us why, unfortunately, most folks who are won’t vaccinate know one another.
Note the highest groups are among Republicans and Evangelicals, collectively amounting to more than 40% of either not vaccinating or needing for it to be required. It is likely that many of these folks attend the same churches, belong to the same or nearby communities, and will otherwise engage with significantly less regard or no for interventions like mask-wearing, social distancing or extra hand-washing. (46% according to the same KFF Vaccine Monitor) Making it more likely that if they are infected, that they may spread it to others who are also not following interventions.
We’re familiar with this problem it exists in the US in a variety of ways, In 2017, Minnesota’s Measles outbreak was due to a Somali-American community being fooled into opting out of the MMR vaccination. Granted, the vaccination rate among the group was as low as 41% among children, its important to consider that outside of this group the vaccination rate is likely near 95%+ for neighboring communities. If the community intermingles with other anti-vaxx communities they bear the risk of spreading it further, or worse trading it back and forth between groups who are similarly unprotected against the virus.
The reality of new cases going forward is this, in Seattle early June 2021, they found that 97% of cases had occurred in unvaccinated folks. It’s worth mentioning that when vaccinated the likelihood of symptoms and severe COVID-19 is significantly reduced due to it being a protective vaccine, so it is highly unlikely that even if a vaccinated individual came down with symptoms that they might even go the hospital or even be tested without a severe response. In addition more folks with less severe symptoms are less likely to be counted among cases as they’re likely staying home following best guidance.
That being said, it means that unvaccinated folks are where the virus will live, and where it will evolve, and the tight-nit anti-vaxx communities are ripe for being reservoirs.
With this information in mind, lets revisit the title again: When captors masquerade as allies.
The Fault in our Stare Decisis
Anyone paying attention can clearly note that folks who might be vaccine hesitant, by nature, aren’t necessarily allies to Spoonies who live with health conditions limiting their daily lives.
When someone with a health condition needs accommodation to be able to enter, use, or otherwise act in an equitable legal fashion in a public space, or space available to the public, the ADA is often invoked. When someone is employed, and an employer seeks to unfairly punish an employee due to the specific conditions or imposes requirements which make the employee unfit for their role, the ADA can be invoked. If you’re interested in learning how the ADA came about, it’s a ton of activism.The Americans with Disabilities Act is a tool for folks with legitimate disabilities to help the world become a more equitable place. It allows folks who might otherwise be excluded, an opportunity to be included. Additionally, another law often utilized by Spoonies, patients or folks with disabilities, is Health Insurance Portability and Accountability Act or HIPAA. For school children FERPA might also apply, but that’s a whole ‘nother bag of worms. HIPAA protects records from being used against us, by securing them, otherwise it would be likely that employers, insurance, and even hospitals themselves might use this data is other ways. By securing privacy of health information, It prevents stigmatized conditions from discrimination, prevents insurance from specifically coordinating with the employer to charge you more, prevents hospitals from profiting off the data by selling it to pharma/med device/tech companies. You don’t have to disclose your health status, because of a complex interpretation of the constitution by the Supreme Court regarding the right to privacy, but it won’t help getting out of wearing a mask or not being asked about vaccination status. Specifically Griswold v. Connecticut (1965), Eisenstadt v Baird (1971), Roe v. Wade (1972), and Lawrence v. Texas(2003) are generally the cases which really cement the Right to Privacy.
These two laws, in concert with the Stare Decisis (Court Opinions regarding legal situations involving these laws which expands or modifies their interpretation) of courts in regards to them, create the legal shields which help some folks stay employed, work, live, seek education, or simply interact with the world.
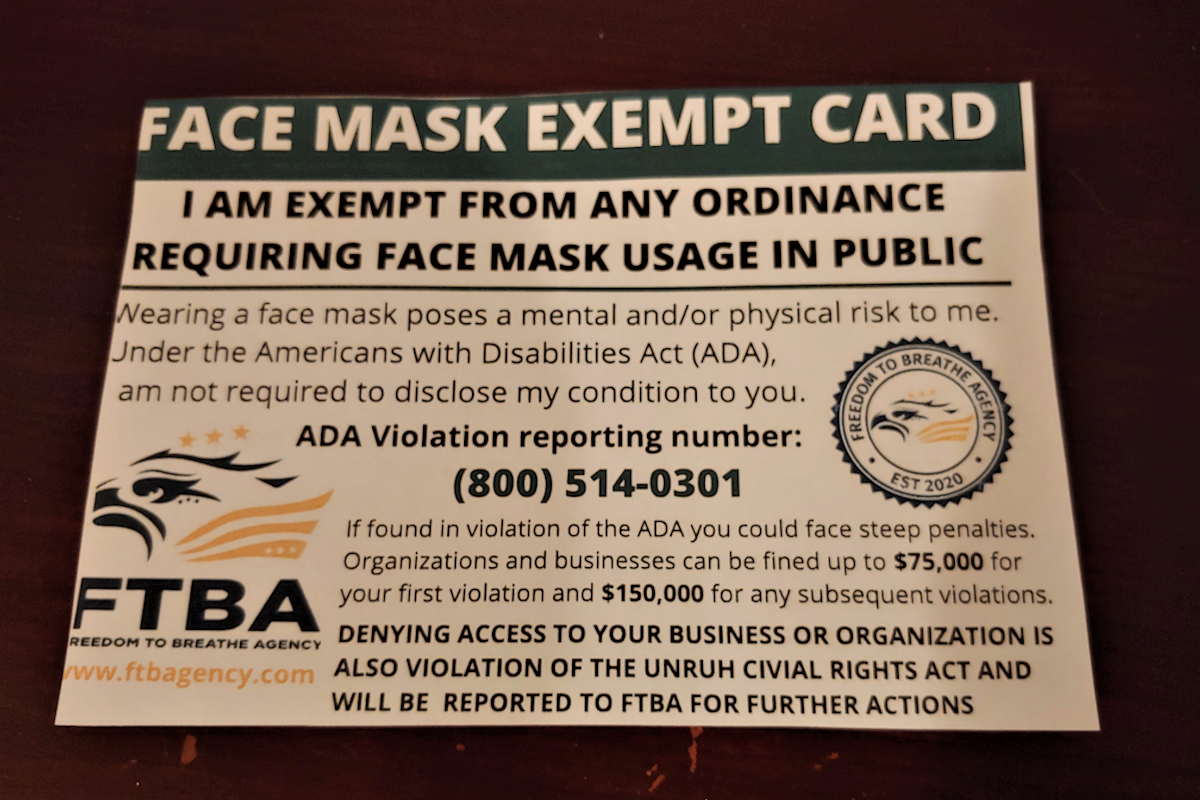
As many who might want to ignore rules for their own personal reasons, might seek to misuse these protections, to shield themselves from responsibility. Over the year+ of this Pandemic, multiple different clearly fake cards have been produced claiming that these two laws would allow the bearer the ability to ignore Public Health protocols being privately enforced by businesses, or publicly enforced for national security, when they most certainly do not.
While they might wield the ADA and HIPAA like a club, they masquerade as folks who need it. Now, as the vaccination effort approaches a critical juncture, we see this same poisonous-allyship. To avoid personal responsibility, a handful will pretend to be spoonies. But even when they do not masquerade, the reality of their not taking the vaccine means a lower likelihood of community immunity, and they remain captors of folks who have no choice in the matter.
I wish this were the end of the part about anti-vaxx co-opting of the “unvaccinated” category, but sadly TikTok has become a strange place for anti-vaxxers to have a new trend. From the hunger games “I volunteer as tribute” phrase and salute to even using the mocking Jay whistle. This is much like the opposite of those attempting to masquerade as allies, but here instead as unvaccinated spoonies being lumped in with their “solidarity” for being unvaccinated. For Spoonies who have no other alternative to being vaccinated, or for Spoonies like myself where the vaccine is less likely to work, this is beyond insulting. We already advocate for real health problems, we don’t need this weird diversion of focus.
As spoonies we must wait for community immunity or the virus to become a minimal threat and no longer endemic to a region. Both of those are tall orders right now given those who would masquerade as allies are now effectively holding us captive, as for many of us spoonies with immune-issues will continue on as if it were still rampant, for we were the vulnerable population before the vaccine’s availability, now we could end up being even more so.
Unfortunately last month the CDC announcement of their new mask guidelines began a terrible trend. The CDC recommendation ignores evidence of transmission from vaccinated folks being similar to that of asymptomatic cases.Why is that concerning?
Asymptomatic and pre-symptomatic cases have been the dominant method of the last year for transmission. ” transmission from asymptomatic individuals was estimated to account for more than half of all transmission” This predominantly due to our minimizing interactions, use of symptom checkers like thermometers, and mostly because folks who felt ill were told to stay home and given additional sick days to accomplish this. So now, as we move about again, and the majority of folks, functionally become like asymptomatic cases, are less likely to be tested because they are vaccinated, and are less likely to feel unwell, prompting less caution regarding transmission. Public health experts have repeatedly gone out of their way over the past month to explain the necessity of these masks after vaccination, and a recent study highlights these points. And with the data that we’re seeing here, with so many folks not vaccinating, The CDC mask policy only makes unvaccinated folks more vulnerable. So to see that Cal/OSHA, Newsom and the lot of them caved again to “business leaders” AKA Big business is absolutely unconscionable for a number of reasons. And to cave in an odd way, to no longer recommend that workers, even in high-risk jobs, wear a mask is likely due to additional pressure from the recall campaign.
1. Pandemic still raging around the world, importation risks remain high, especially with new VOCs.
3. The tests still kinda suck! Due to the windows of false negatives no current test breaches about 60-80% in sensitivity aka false negative rate. The problem is the way the virus does it’s thing compared to the administration of the test on the patient timeline, some more sensitive tests exists, and saliva testing has shown to be more robust in early detection than more typical NP/OP swabs.
4. The CDC mask guidance dropped months earlier than it should have, using them as guidance to make things consistent has nothing to do with health, rather with consistent regulation showcases our Safety 3rd mentality regarding health regulation.
5. When we consider the rates of potential folks who cannot vaccinate alongside the folks who will not, these numbers make community immunity potentially our of reach, especially with continued importation of cases, which can see more clearly with VOCs. All of these decisions seem quite premature.
In situations like this, caution is the better decision, moving slowly, with available data.
Right, Rick, but how does this affect you personally? I’m a transplant patient, who is planning my vaccination with my doc, it means waiting more than I’d like, it means seeing those around me start to engage in a slowly opening world. It means saying no to networking opportunities, potential career-boosting opportunities, and a great deal of advocacy. It means having limited interactions with friends and family even though the vast majority are vaccinated. Having close family members who are also in the same Spoonie boat, increases our vulnerability. I’ve already spent 6 years in end stage liver disease and the last year damn, I know the fear and potential pain many in the community sense or feel. Unfortunately the vaccine may not even take due to my immunosuppressant meds and in the rare event that my antibodies are detected, it is not recommended as a confirmatory test on immunity.
But while SD county only has about 19% of its population unvaccinated currently, neighboring Imperial County has about 32% of its population currently unvaccinated. You san see County by County data here.
Red represents conservative leaning counties, San Diego still slightly leans conservative.
These percentage points, combined with the reality of growing interstate travel and vacation use, means as a tourist destination, San Diego is also likely to see more importation cases from neighboring states with less regard for health and safety. So while San Diego folks are more cognizant of their health, tourists might not be.
Okay, well that was awful, is there anything that can be done? Or are we just fucked?
I mean, for those of us in the spoonie community, we know how common the latter is, but in this case there is more that can be done. While states give away money, or Xboxes, cars, or whatever else seems clever, the reality is that folks who aren’t interested aren’t likely to be swayed by a SWOT analysis. They’re likely to be influenced by their peers. Some “Maskueraders” won’t understand so easily and it may take time for them to understand the real risk and adjust their worldview. Patience and tolerance is important.
If we want to be free again in this country, in this world, we must be prepared to protect our community, our nation, and our world, by at the least getting a vaccine for COVID-19. It probably would also help if the federal and state governments could agree on a standard for ensuring vaccination, like having some kind of universal database (it exists with HHS already it’s just not connected to anything outside of a few departments) having at the very least a robust nationwide Electronic Health Record system would help in every health fight, improve mobility within systems, reduce administrative costs, streamline costs/billing and further the goals of health equity in the American population.
In the meantime, please wear a mask when around others in close quarters, or in mass gatherings/mass transit, and if you aren’t yet vaccinated and can get it, please do and encourage friends and family to do the same.
TLDR: Vaccine rates won’t go down unless we talk to our friends, family and neighbors and make sure everyone who can vaccinate does. The CDC Mask policy makes the pre-emptive reopening potentially worse, and worse for unvaccinated folks who account for nearly all cases in the US. Anti-vax folks pretending to be disabled doesn’t help anyone. Blending the category of unvaccinated conversationally benefits anti-vax movement, as they pretend to be martyrs (who don’t think they’re going to die? it’s confusing) Expanding poor health policy only further erodes what little public health trust exists in institutions. We can always hope it’ll turn out alright, but as a six time survivor of Hep C treatments, my caution regarding Epidemics is imbedded.
Johansson MA, Quandelacy TM, Kada S, et al. SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA Netw Open. 2021;4(1):e2035057. doi:10.1001/jamanetworkopen.2020.35057
La Marca, A., Capuzzo, M., Paglia, T., Roli, L., Trenti, T., & Nelson, S. M. (2020). Testing for SARS-CoV-2 (COVID-19): A systematic review and clinical guide to molecular and serological in-vitro diagnostic assays. Reproductive Biomedicine Online, 41(3), 483–499. https://doi.org/10.1016/j.rbmo.2020.06.001
Patel MD, Rosenstrom E, Ivy JS, et al. Association of Simulated COVID-19 Vaccination and Nonpharmaceutical Interventions With Infections, Hospitalizations, and Mortality. JAMA Netw Open. 2021;4(6):e2110782. doi:10.1001/jamanetworkopen.2021.10782
In 2014, while almost three years into end stage liver disease and recovering from c.diff (clostridium difficile colitis for those imbibing their daily Latin) it’s transferred via fecal-oral, so when someone doesn’t wash their hands making food, and unfortunately it dries ya out distributing one’s contents most expeditiously through the major available routes.) , I was in a strange space. I knew that the end might be coming soon, and when I was told that if my vitals (my INR was almost okay but my Bilirubin was stupid high) didn’t improve, I would likely be brought to the liver transplant floor at my other hospital.
I remember not being allowed to leave the room except with another person with me, I remember walking with a friend of mine, who had a heart condition, and together with another spoonie friend with severe lupus we called ourselves “lifers” due to our likelihood of shortened lifespans. I was diagnosed with Hepatitis C at age 12 and told by 30 I would likely need a liver transplant or die. (And he was pretty freakin’ close.)
Hospitalized in 2014
I saw my reflection in the glass in the garden I wasn’t allowed to go into. It was distressing visualizing the reality of my more imminent potential demise.
We spoke of the fear, of the reality ahead, that I would likely wait for weeks in the hospital, in this situation. I wasn’t quite dying just yet, but my liver’s Model for End-stage Liver Disease MELD Score had jumped into the 30s. which meant I was nearly a candidate for liver transplant, and my liver would soon need replacement. There were no guarantees, a person dies every ten minutes waiting on the transplant list in the United States. (btw register to be an organ donor today, save a life or 8 donatelife.net)
I didn’t entirely know what to do, and when my friend left, I started looking for solutions. Being a patient for as long as I had, and having just started writing about my experiences, I felt it important know everything in power about my condition, so that I could better explain the road ahead to others. So that night, I researched, I had found that bilirubin was not only the primary reason for my Simpson’s skin tone I was rockin’, but also my constant itching. And more importantly I’d learned that when babies are born and have high bilirubin or show jaundice, they put them under a UV/Sun lamp, because it helps break down bilirubin. That had to be it. My INR(clotting factor) and bilirubin(liver stuff) had not budged since they plateaued on day three of my stay. But I was convinced I had found a solution. I spoke to the nurses, explained I wanted to go for a walk outside the hospital. It took an amount of conversation before they were amenable to my request, but with a CNA, I was allowed to walk around outside. Then later I repeated this, until I was walking outside for about 40 minutes per day during peak times of UV (10am-2pm for the curious), at 11am, and a little before 2pm. My bilirubin began to drop by day 5 in the hospital, and I was released on Day 7. My research had paid off, I was able to better understand the circumstance and ensure my own improvement. Something I could do for others with the hindsight of my experience, but this, helped me decide I wanted to learn how to research better. I wanted my Master’s In Public Health.
For the next two years, every doctor’s, outpatient procedure, hospital visit I had I absorbed everything, every question I could ask, every thing I could learn, and naturally, I would reflect my interest in earning my MPH. It also gave more meaning to my family’s and my exhausting terrible journey, it let me turn a stigmatized and debilitating disease, into a badge I wore with distinction. In 2016, when NoHep2030 Launched, it only further added to my new goal: Help Eliminate the disease which had nearly killed me and my mother. I found purpose.
2016 was a year filled with so much, from the launch of NoHep, to my advocacy efforts in Sacramento, to one of my best friend’s weddings, and unfortunately, not long after, I became too sick to treat. July 2016, My liver damage was too far gone, without a transplant soon, I would likely die within the year, and certainly by a years’ time. The stress and uncertainty that befell my family and friends were challenging, they would help me see that my resilience was bolstered by their own. I had accepted my likely imminent death, and hoped and persisted in living as best as I could. My mother’s guilt, wore heavy, and words can do little to describe the hollow feeling in my family of the grim reality ahead. But after years of grueling, waiting, in the beginning of December, my family received the best Christmas gift we could have ever wanted. I received a liver transplant.
Liver transplant with my surgeon
After my transplant, I was to be on Disability and Medicare+Medicaid for about two years following the slow recovery. Disability has an amazing program called Ticket-To-Work, it allows the person who uses it to not only cover the cost of their education, but continues to pay the same disability and most importantly delays disability hearing until after graduation (Disability hearings are rarely won, of folks I know who have tried, two of twelve have been able to remain in the program.) This would have allowed me get my MPH, and get a well-paying job after graduation, and rise up out of the under-the-poverty line life of disability.
After my transplant my Hep C came back with a vengeance. It skyrocketed to over a hundred million, (for reference like 10 million is really high) and it would not be long until my new liver was reinfected. The treatment was quickly approved, though off-label, it was the only possible combination which could have solved my unique variant strain of Hep C. I’d suggested a similar combination of meds a year earlier, but had become too sick to treat before one could be attempted.
The treatment is its own story of chaos, denials, appeals, near lawsuits and a go-fund-me page, but ultimately I wouldn’t find out the result of the treatment until September.
GoFundMe for my sixth treatment
During the chaos of my sixth treatment for hepatitis C, I’d also applied for the MPH program at Cal State University San Marcos, I spoke with my colleagues in patient advocacy and friend’s mom who had been a preceptor(people to look at candidates to a program) for SDSU. I was surprised to find out that my application to the program had been rejected. My letters of support were good, my essay was heartwarming and thoughtful, I was at a loss for why.
Being honored at the 2017 Liver Gala as their Liver Champion and 2017 Liver Activist for American Liver Foundation, pic with my awesome docs
Until I remembered something. When I graduated CSUSM in 2009, I had a 2.89 GPA, high enough for the 2.5 GPA threshold of the MPH program. However, after I graduated, I worked for a School District for 39 hours per week. This was pre-ACA, so I had no option for insurance, and with a preexisting condition, losing my insurance meant, I could be denied health insurance and thus treatment, if I did not maintain my health insurance. With an economy in shambles, my only option was to continue going to school after work, halfway through my first semester I began my at the time second treatment for Hep C. It was brutal, and the long hours along with school would discourage my application to many of these classes. The resulting Ds and Fs on my record from this time, were now interfering with my ability to enter grad school. I’d explained the circumstance, and that my grades following my graduation do not reflect my ability as a student, but the necessity of my livelihood in a broken health insurance system. This wasn’t enough. In order to get into the program, I would need to expunge these bad credits. It would be impossible to hunt down the 10 or so likely adjunct professors from near seven years prior, I needed a better solution. I found one in academic renewal, by taking 30 new credits I could wipe out 30 bad credits and improve my Cumulative GPA.
While I’d lost a step, having been in end-stage liver disease for over five years, and living with hepatic encephalopathy for as long, I’d resolved that my experience at Community college would tell me if I were capable of doing what I’d dreamed of, earning my MPH, writing my book, and helping to eliminate Hep C. Classes took a moment to refamiliarize myself, I was able to cover school thanks to the California promise grant. I aced through community college, taking a few fun courses like Ceramics and genetics, and some more challenging ones like statistics and a social media marketing. But when I’d applied again, my academic renewal had not yet gone through, causing the same rejection from the school, which would postpone my entrance until 2019. Each time I applied I added more recommendation letters, and referenced more of the advocacy work I had been doing during this time (I was working for Help4Hep, writing for Hepmag.com and HepatitisC.net, had started working for UCSD as a patient stakeholder, and was doing a lot of public speaking.)
2019 Patient advocacy pictures
In 2019, a few months into my new job, I was accepted into the MPH program at CSUSM. I was elated, finally, I could take the first step I’d been wanting to take to help join the fight to eliminate Hep C.
So it turns out working full time, and doing an accelerated masters program at the same time, is a quite time-intensive and stressful. Doing this during the pandemic, was even more challenging, let alone when my thesis topic is the pandemic. Between the panic attacks, depression, shoulder dislocations, optical migraines, a bout of cellulitis, my thesis Chair having to go out on medical leave a month before my defense, the process itself is also a story for another time. But regardless of all of these things, healthy pacing and preparedness, and peer support helped me carry on.
On April 28, 2021, I successfully defended my thesis. (I can’t show ya it though, I emgargoed it, so I can publish it.) and on May 22nd, I will begin my renewed birth in life.
But I am most excited to share with the world, the good I can do.
I hope to help change how we see patient advocacy. I hope to empower thousands of folks when I am done.
Just as I did in my life before transplant, as a leader of a grant-based 6 to 6 program, and eventual consultant. I do not aim for the moon, I aim for the community I serve.
Often have I searched the internet wondering, where can I find helpful Hep C resources now that HCV Advocate is gone? Well there’s HepMag, Help4Hep (if you need help with treatment give ’em a call!), IhelpC, and HepatitisC.net, but they’re really good tools for information or story sharing, or delicious liver friendly eats(IHelpC). To help provide a space where we can connect with others who have experienced Hepatitis C Virus (HCV) or those who seek treatment, advice, guidance, or want to do more in the community!
This is the HCVME Community Discord It will prompt you to create a discord account. Due to the public nature of the discord, I have required a registered Discord account. Additionally I’ve set up a channel which features the latest from twitter regarding Viral Hep and Liver disease. featuring advocates like myself, but also liver organizations and medical experts. I’ll be on there posting HCV resource information and what not periodically. and come June, I’ll be on the discord regularly for chats! Please join us! make sure to agree to the rules and pick a role with fits you!
In May we’ll be launching the HepChat Hour on Monday evenings Pacific time 5:00pm-6:00pm on the HCVME Community Discord!
As a patient advocate, I often find myself taking a yearly trip (or a few) in the spring to speak with lawmakers and their offices. I speak to a number of injustices. I say this because they’re a strange combination of factors from willful defiance of the law to intentional underfunding likely due to in part to stigma and in part because it wasn’t “actionable” until 2013. Actionable, in this case, refers to investing in something that can improve or have a result which is desired. In truth, the only treatment prior to 2013 was still a crapshoot with a 70% cure rate (this rate does not include dropouts). Prior to 2013, there was little reason for an elected official to care about Hepatitis C (HCV), as little could be done. But in 2013, when a new treatment could help the millions suffering from Hepatitis C, instead, states restricted access to the treatments because they were expensive. (In truth if every American with HCV were treated for HCV with those prices, the numbers would run in the trillions, as it was about 88k per treatment and HCV affects between 3-6 million Americans. But due to the structure of healthcare here and the fact that more than 50% of people with HCV in the U.S. are unaware of their status, that could never have actually happened.) But when the prices fell, some states maintained the restrictions, some even expanded them. In 2015, CMS(Centers for Medicare and Medicaid Services) stepped in and issued a memo ensuring that all state Medicaid offices should not have restrictions for HCV meds. Despite both the significant decline in cost of the medications and the mandate of the 2015 CMS reiteration, 11 states continue to use liver damage restrictions, 34 states along with D.C. and P.R. continue to use sobriety restrictions, and 27 states along with D.C. and P.R. continue to use prescriber restrictions on access to Hepatitis C medications. In Texas, a Hepatitis C patient must be permanently injured with cirrhosis before they can access treatment. These restrictions are illegal, yet they persist. If you want to see a great breakdown of just how bad this is.
The State of Hep C with Medicaid Access (courtesy of StateOfHepC.org)
Something as simple as an additional memo from the White House to CMS, giving them the ability to enforce the coverage and encourage Managed Care Organizations (Insurance organizations but for Medicare/Medicaid) to remove the restrictions might help ensure access to Hep C medications in states like Texas. An uncharacteristic hyper-regulated health access policy stance possibly due to strategic ignorance under the belief that it is more thrifty to deny live-saving medications to their residents. If you live in Texas, Montana, South Dakota, Missouri, Nebraska, Iowa, Indiana, Alabama, or West Virginia, have Hep C and are in need of assistance, please check out Help4Hep, give ’em a call they’re a great group with helpful resources. Otherwise, maybe find your representative and tell them how absurd this is?
The other matter also involves a certain ignorance; however, this one does not have the willful defiance fueling needless death. Hepatitis C has been chronically underfunded for decades. It currently is funded at 39 million at the federal level. That’s about 12 cents per person for the entire United States. For a condition which affects between 3-6 million Americans, and an additional 1.2-2.2 million with Hepatitis B, it is painfully surprising how little funding has gone into helping patients with viral hepatitis. I recently learned in preparation for a meeting with a house rep, that we lack significant analysis of viral hepatitis as federally, there is only one part-time epidemiologist for all of California’s nearly 40 million residents regarding viral hepatitis.
Virtual Hill Days have temporarily replace typical Hill visits
Right now, NVHR, Hep B Foundation, Hep B United, NASTAD, and others are hoping to expand the budget for viral hepatitis. The CDC has estimated that it would require an annual commitment of at least 316 million dollars to put the United States on the path towards viral Hepatitis Elimination. The current suggestion is to increase the budget to 134 million, less than half of what the CDC estimated is necessary. While personally, it’s disappointing to imagine a world where people disagree with public health priorities, we have positioned ourselves for modest but strategic gains in funding in this decreased ask. Because at 134 million, that’s still less than 50 cents per person in the United States.
This funding would expand one of the most critical elements of Viral hepatitis elimination, screening. In 2020, the CDC finally expanded screening recommendations to all adults and rescreening people who use injection drugs and during each pregnancy. While the latter has been met with some resistance from OBGYN groups, the other recommendations are slowly being implemented across insurance networks. (this is why OBGYN groups are misguided in their approach) This new recommendation is meaningless without expanded testing, especially in communities disproportionately affected by Viral Hepatitis. That testing is naturally limited by the current meager national funding. State and local efforts have a hard time gathering support without grassroots groups due to the silent stigma of Viral Hepatitis. Enhancing funding for screening in Federally Qualified Medical Centers and other community clinics would expand the reach of Hep C diagnosis into the heart of the #MissingMillions and start to help people where they are. But screening is only the door; it’s important that folks and doctors are ready to help guide and link patients with hepatitis c to treatment and ultimately cure/elimination.
2016 I joined with CalHep to help expand linkage-to-care.
In 2016, CalHep, formerly a program for Project Inform, now a part of the San Francisco Aids Foundation, led an effort to have several targeted linkage to care programs for Hep C in California. In total, the program was successfully funded for three years, with two million going into primarily three linkage-to-care or physician-education programs. It was very successful, but ultimately it would not be extended in 2018 due in part to Gov. Brown’s stance on long-term funding. This program’s total cost was roughly 6 million dollars. This is a familiar figure to me, as my bill to insurance total sits at a bit over 6 million dollars for all of my care as a Hep C patient since diagnosis. Efforts like CalHep are scattered throughout the country and have been empowered by local campaigns like End Hep C S.F. and Hep Free NYC. These grassroots groups are the backbone of Viral Hepatitis elimination in the U.S., and are in place ready to be empowered by increased funding. Groups like Hep Free Hawaii, like End Hep C San Diego, work as private-public partnerships with stakeholder groups. Most elimination campaigns are paired with or work with local Harm Reduction groups. This is a natural fit, as there is no way to eliminate hep c without addressing its most common transmission route, intravenous drug use. Harm Reduction groups add to the grassroots power of Hep C elimination. As folks at End Hep S.F. have seen, when people are cured of HCV, they accomplish secondary goals and may have an easier time controlling their substance use; it is an incredible state change being free of viral hepatitis, an otherwise death sentence. Grassroots organizations aren’t just here in the United States, NoHep is worldwide; as a program from the World Health Organization and World Hepatitis Alliance, it serves to connect and share data with micro-elimination movements around the world. This is our time to come together and end viral hepatitis. We have the tools: Vaccines for Hep A and B, and Curative treatments for Hep C; we have the people willing to do the work, now we need support.)
You can help. This year, Congress is poised to pass healthcare legislation that can improve the lives of millions of Americans. Allocating $134 million for the CDC Division of Viral Hepatitis and $120 million for the CDC Infectious Diseases Consequences of the Opioid Epidemic Program in Fiscal Year 2022 appropriations budget would bring us one ACTIONABLE step closer to Hep C elimination. In 2016 the USA joined in the WHO NoHep Pledge for global elimination of Viral Hepatitis by 2030, but it’s fallen short so far and taken years to take simple steps like universal screening for Hep C, while Hep B still needs universal screening recommendations from the CDC. This funding step would be the first real investment made by the United States’ federal government towards Viral Hepatitis elimination in the U.S. Let’s end Viral Hepatitis.
PS it wouldn’t hurt if we fully got rid of the federal ban on funding Syringe Service Providers, it would provide a helpful destigmatizing avenue for people seeking treatment.
We had just wrapped up a three day conference for Help4Hep, and I was wearing a shirt, a shirt I originally wore for a press conference against the BRCA.(The awful replacement for the ACA on the senate floor last year.) A form fitting black cotton T-shirt that reads: “Hello, My preexisting condition is Hepatitis C.” The shirt’s purpose was to bring to people’s attention two things: One that Preexisting conditions aren’t really visible, but they are common, and Two, That Hepatitis C is among them, and I have it. Even while being cured of Hep C, in the eyes of the medical world and insurance I will forever be a Hepatitis C patient.
Maybe it was because I was standing alone before we boarded, maybe it’s because I was visible, sitting in the front, but regardless why the next series of events happened, it’s unfortunate that they did.
I wear a mask because I’m immunocompromised due to Liver Transplant
I was seated in the front row, and I was talking with the lady seated next to me about hepatitis C. My shirt was a conversation starter, earlier I’d explained the prevalence and the cure to a few others who’d asked. She was explaining to me that her mother had it and we spoke about the cure, to which she seemed surprised, but often people are unaware of it, so I went into more detail. I explained that there’s a lot of ignorance around the virus, and the cure, largely due to stigma about even talking about.
“Excuse me sir, I’m going to need to talk to you.” The flight attendant interrupted. He and another attendant pulled me off the plane and onto the boarding ramp. he began ” A passenger expressed concern about your shirt, could you explain?” Without thinking I responded I’m a Hepatitis C advocate, I just came from a conference. Noting their faces unchanging waiting for more information I continued. There’s a lot of ignorance about the disease, and a large part of that is due to stigma, so I’m not surprised someone is concerned. They asked if it was an issue.
And I responded, unsure if they meant an issue for me or for them, as the situation implied they took issue. “It’s a blood borne pathogen, it’s blood to blood only,” I continued, still waiting for a response I explained that I was cured last year, but regardless this shirt is my status, and it’s not an issue. I’d had enough of their concerned faces, and turned around and went back to my seat.
I was far too aware of the level of control airlines have over passengers, and now being a transplant patient I only had so much medication with me, so being stuck there was a concern.…
It seems insane that something so necessary could increase in price so much over a short period of time, but Healthcare premiums have doubled in most states since 2013.
What’s worse is that for some states; Alabama, Alaska, and Oklahoma, it nearly tripled. The ACA’s three tiered structure was created to eat some of those cost increases and ensure that insurers had access to a larger market. The individual mandate helps keep prices from ballooning faster. And the premium credit gave those with low income, access to the market. The ACA was installed to slow the growth of premiums, and yet it outpaced inflation by more than 95%, this often leaves most consumers wondering…why?
There are a number of reasons for insurance premium increases, one has to do with the way companies responded to the ACA. Many retail employers began spreading out workers, opting for more employees, lowering the amount of workers available to receive full-time benefits, Ironically mostly in government-based hourly jobs. Companies began going for less Cadillac plans and focused on silver packages, which caused a sudden surge in middle package buying, increasing the prices overall. But company reactions were a drop in the bucket compared to the next two components.
An aging market
As boomers grow older, their health demands rise; and while hospital use is up, nursing and doctor shortages can create three to four month long wait times for appointments. Boomers’ reliance on pharmaceutical medication outpaces any other generation. Medicare spending in 2015 was $137.4 billion on prescription drugs in 2015, up from $121.5 billion in 2014. Medicare Part B spent $24.6 billion on prescription drugs in 2015, up from $21.5 billion in 2014. A whopping $7.03 billion was on Hep C meds alone which cured maybe ten thousand people, and with nearly 5 million Americans needing treatment it’s easier to see why premiums are rising. But it’s not just meds they need. Surgeries and outpatient services ranging from colonoscopies to knee replacement are up across the nation as our nation ages.
Pharma Bros:
Valeant Pharmaceuticals’ Ativan increased by more than 1,264 percent, accounting for $5.3 million in Medicaid drug spending;
Turing Pharmaceutical‘s daraprim increased by 874 percent, accounting for $16 million in Medicaid spending; and
Hydroxycholoroquine sulfate increased by 489 percent.
Each of these increases doesn’t reflect need by the consumer, nor a need for research in development. The price increases are a measure of market control given to exclusivity of production. Investment firms purchase companies with the goal of milking them for investors as they shift focus to their new number one product: their stock. These kinds of moves produce volatility and increase the prices insurers need to set to control for.
As the individual mandate is now set to disappear in 2019, it raises a serious question, will consumers be able to tolerate Premiums which cost more than their rent/mortgage payments?
What brings us here, to these locked warehouse doors are the restrictions on access from insurers, and medicaid . High cost pharmaceuticals, and the changing of their discount policies. And the lack of effort by governors to approach discounts because of the pending TPP.
I’ve been talking a lot recently about these things and how we get to here.:
The Locked Warehouse Doors.
if you were denied Sovaldi, Harvoni, Viekira Pak, or any other new HCV med, if you had to go through lots of hurdles for treatment; I urge you to tweet/post about them with the hash tag: #LockedWarehouseDoor.
What Happened to My Support Path? Gilead used to offer My Support Path to larger audience, but they’ve clamped down on the discount in hopes of allowing more patients access to their meds by pressuring insurance companies to loosen restrictions.
Medicaid’s Silenced Epidemic
Medicaid’s inability to assist the needs of HCV patients in many states unless they have permanent liver damage and depreciating quality of life. These restrictions are in place even thought preventative treatment would cost half as much.
The Trans-Pacific Partnership
An agreement that could worsen the already steep drug prices we have, and limit the power of insurance companies/Government based Health Insurance like Medicaid to get discounts.
Medical Tourism as Bad Tourist Behavior And how Developed Countries are hurting themselves and LDCs(formerly third world) when patients mess with the supply of Live saving inelastic goods.