


As of June, 2021, I will have been eligible to get the COVID-19 vaccine for over four months now as a Solid Organ Transplant Recipient. I am a person who received a liver transplant, younger than the average at the age of 35. My transplant journey is a rough story concerning my life-long battle with Hepatitis C, six treatments, and six plus years in End-Stage-Liver Disease you can read more about the story here.
Because this story isn’t about me, per se, but about the circumstance that I find myself in, along with so many of my peers. Before I explain further all of this, some background is in order as to explain the importance of understand the nuanced differences in vaccine hesitancy and folks who are among the “unvaccinated”.
I belong to part of a large group of vulnerable folks, collectively, spoonies is the best term here. Because the complex mix of auto-immune, genetic, medically induced and viral infection induced immune responses include lots of folks. From folks with certain cancers, folks with HIV, to folks like myself who take medication which suppresses our immune system.
Collectively it’s estimated that we comprise about 4-7% of the United States population, with about 2.7% of the population being transplant recipients like myself.
Many of us who might benefit less from the vaccine, will continue living as if nothing has changed. Masking regularly indoors, outdoors in groups, increasing our hand-washing and keeping some physical distance from others, especially if near crowds, and minimizing interactions.
There are many estimations of when Community Immunity may take hold, somewhere between 70-90% is the average of all the literature and articles I’ve come across. In Brazil, the efforts to induce natural herd immunity, in part by relaxing non-pharmaceutical interventions like mask wearing, resulted in the population of Manaus having as many as 76% of the population infected, and also provided us with the P.1 Brazilian variant now being referred to as the Gamma variant. So to be at the the functional level needs to rely more heavily on vaccine induced immunity, in part because it potentially lasts longer. More importantly it is more robust than natural immunity as more documented cases of reinfection have occurred through natural immunity, especially in regards to Variants of Concern. And it slows the potential for new variants due to significantly reduced levels of viral procreation when vaccinated. (aka less viral load in vaccinated folks means less potential for evolution into new variants, because it doesn’t generally evolve in the wild, just in people/animals.)
As Variants of Concern continue to appear due to the uncontrolled and widespread state the pandemic is currently in, we must consider that these will eventually impact transmissibility of SARS-CoV-2., as both the Alpha variant (AKA UK variant AKA B.1.1.7 variant) and the Beta(AKA South African Variant AKA B.1.351 Variant) have. How this in turn is met with growing vaccine uptake, time is slowly revealing.
For those not familiar, this is the Kaiser Family Foundation Vaccine Montior. An important constant pulse on vaccine uptake and trends here in the United States. Crucially, it has been monitoring the Already got it vs ASAP vs Wait and See vs only if required vs Definitely not.

Within the Spoonie communities some of us may attempt to get the vaccine, anecdotally, many who have reported higher than average instances of side effects, or no effect whatsoever. For others in the Solid Organ Transplant situation concerned about the vaccine check this out, it won’t help you make your decision, but it might help inform it a bit more, especially if you check their references.
Now for the reference to the title of this piece, who are these captors?
The vaccine hesitant for non-medical reasons, and most importantly those who would refuse themselves and their children the safety of a protective vaccine.
For spoonies like myself who long for a return to seeing friends and family, going to a graduation, a wedding, even a funeral, there is little hope in reaching community immunity without the help of those who also fall into haven’t gotten the vaccine category. For veterans of the spoonie community, we’re no strangers to phonies, con-artists, scammers, and conspiracies, especially on the internet, not to mention the people who call them out, and people who accidentally call out real Spoonies. When you achieve a certain level of fame on Instagram, some spoonies find themselves fighting off fake accounts, copies of their own who grift unexpecting folks. We’re used to folks pretending to be disabled standing next to us in line for a Disability Access Pass in Disneyland, or folks who claim medical exemptions for hardships where none exist. And we’re used to the increased scrutiny and disbelief of our condition if not visibly apparent. For some it reinforces imposter syndrome, it encourages them to avoid seeking help, there are layers to these problems which are important to know exist as we explore the reality for folks like me in 2021 in regards to vaccine hesitancy.
The alarmingly high number of 13-15% of folks answering definitely not to the vaccine likely includes a small portion of folks like myself to more extreme cases who absolutely cannot get any COVID-19 Vaccine. But even without considering that, we can be assured that this % is not consistent state-by-state, and significantly different between rural and urban populations.
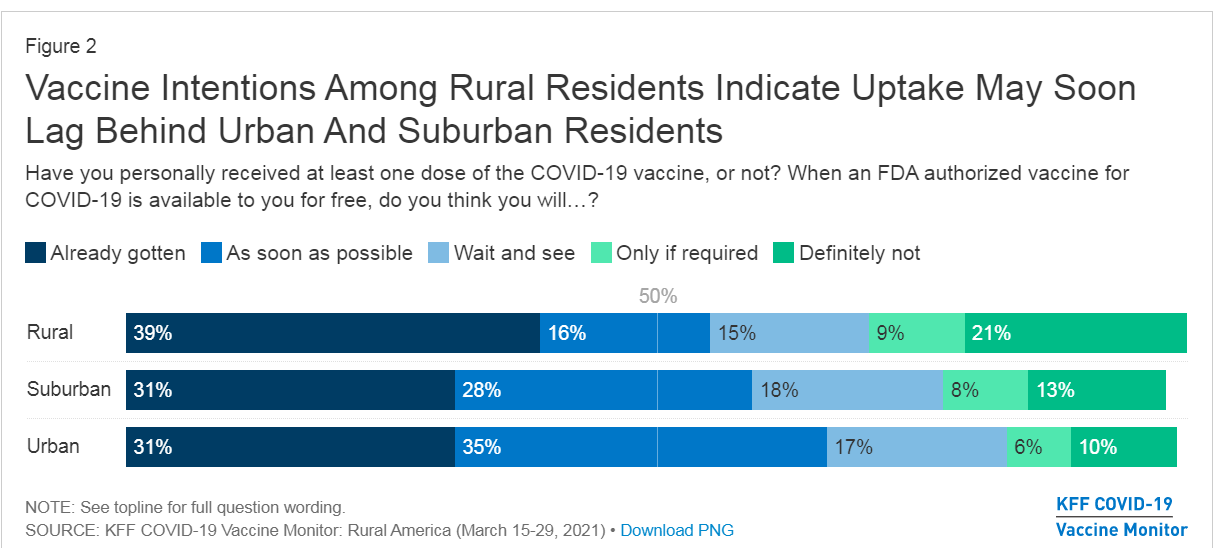
We see that among rural populations, the majority of folks who would not be vaccinated number as high as 21% on average. It is impossible to extract from this data where spoonies might fall. Because some of us have already gotten the vaccine, many like myself wait and see, and some already know they cannot take the vaccine, or are so alarmed by side effects they’ll only do so if required, and even then they may quit or be fired.
Let’s assume the upper limit of 28%, a stat where every spoonie cannot vaccinate, with a lower limit of 23%, where only a few spoonies vaccinate successfully against SARS-CoV-2. It means that on average among rural populations the vaccination rate might not breach 72-77%, clearly around or below the 76% which existed in Manaus for their attempt to gain Herd Immunity. Again, Vaccine Induced immunity is likely stronger against SARS-CoV-2 and its VOCs, but at such low rates of vaccination, it poses a significant danger in a different way: Reservoirs. Reservoirs (of infection) are individuals, animals, plants, substance, soil or a location which the virus lives and multiplies. Reservoirs make it hard to eliminate an epidemic, in the U.S. and other countries the prison system does this with Tuberculosis and Hep C. As populations in the prisons have significantly higher incidence of disease than populations outside prisons. Reservoirs don’t’ work well if those folks aren’t intermingling but unfortunately…
Another chart form KFF tells us why, unfortunately, most folks who are won’t vaccinate know one another.

Note the highest groups are among Republicans and Evangelicals, collectively amounting to more than 40% of either not vaccinating or needing for it to be required. It is likely that many of these folks attend the same churches, belong to the same or nearby communities, and will otherwise engage with significantly less regard or no for interventions like mask-wearing, social distancing or extra hand-washing. (46% according to the same KFF Vaccine Monitor) Making it more likely that if they are infected, that they may spread it to others who are also not following interventions.
We’re familiar with this problem it exists in the US in a variety of ways, In 2017, Minnesota’s Measles outbreak was due to a Somali-American community being fooled into opting out of the MMR vaccination. Granted, the vaccination rate among the group was as low as 41% among children, its important to consider that outside of this group the vaccination rate is likely near 95%+ for neighboring communities. If the community intermingles with other anti-vaxx communities they bear the risk of spreading it further, or worse trading it back and forth between groups who are similarly unprotected against the virus.
The reality of new cases going forward is this, in Seattle early June 2021, they found that 97% of cases had occurred in unvaccinated folks. It’s worth mentioning that when vaccinated the likelihood of symptoms and severe COVID-19 is significantly reduced due to it being a protective vaccine, so it is highly unlikely that even if a vaccinated individual came down with symptoms that they might even go the hospital or even be tested without a severe response. In addition more folks with less severe symptoms are less likely to be counted among cases as they’re likely staying home following best guidance.
That being said, it means that unvaccinated folks are where the virus will live, and where it will evolve, and the tight-nit anti-vaxx communities are ripe for being reservoirs.
With this information in mind, lets revisit the title again: When captors masquerade as allies.
The Fault in our Stare Decisis
Anyone paying attention can clearly note that folks who might be vaccine hesitant, by nature, aren’t necessarily allies to Spoonies who live with health conditions limiting their daily lives.
When someone with a health condition needs accommodation to be able to enter, use, or otherwise act in an equitable legal fashion in a public space, or space available to the public, the ADA is often invoked. When someone is employed, and an employer seeks to unfairly punish an employee due to the specific conditions or imposes requirements which make the employee unfit for their role, the ADA can be invoked. If you’re interested in learning how the ADA came about, it’s a ton of activism. The Americans with Disabilities Act is a tool for folks with legitimate disabilities to help the world become a more equitable place. It allows folks who might otherwise be excluded, an opportunity to be included. Additionally, another law often utilized by Spoonies, patients or folks with disabilities, is Health Insurance Portability and Accountability Act or HIPAA. For school children FERPA might also apply, but that’s a whole ‘nother bag of worms. HIPAA protects records from being used against us, by securing them, otherwise it would be likely that employers, insurance, and even hospitals themselves might use this data is other ways. By securing privacy of health information, It prevents stigmatized conditions from discrimination, prevents insurance from specifically coordinating with the employer to charge you more, prevents hospitals from profiting off the data by selling it to pharma/med device/tech companies. You don’t have to disclose your health status, because of a complex interpretation of the constitution by the Supreme Court regarding the right to privacy, but it won’t help getting out of wearing a mask or not being asked about vaccination status. Specifically Griswold v. Connecticut (1965), Eisenstadt v Baird (1971), Roe v. Wade (1972), and Lawrence v. Texas (2003) are generally the cases which really cement the Right to Privacy.
These two laws, in concert with the Stare Decisis (Court Opinions regarding legal situations involving these laws which expands or modifies their interpretation) of courts in regards to them, create the legal shields which help some folks stay employed, work, live, seek education, or simply interact with the world.
As many who might want to ignore rules for their own personal reasons, might seek to misuse these protections, to shield themselves from responsibility. Over the year+ of this Pandemic, multiple different clearly fake cards have been produced claiming that these two laws would allow the bearer the ability to ignore Public Health protocols being privately enforced by businesses, or publicly enforced for national security, when they most certainly do not.

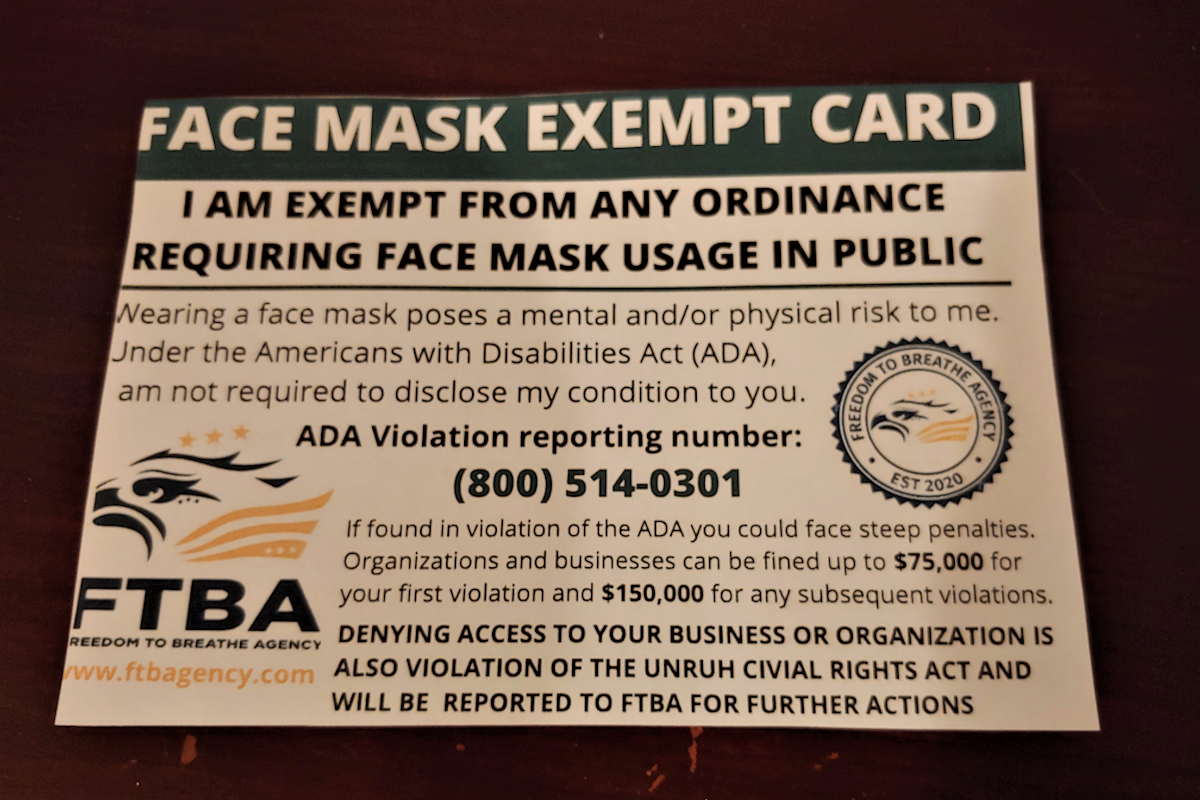
Obviously, these cards are meaningless as the claims on them. But they bring about the next/current reality, Fake vaccine cards and fake vaccine exemptions.
Airlines are now finding this problem to be incredibly challenging to police since there is no official method of tracking vaccination in a way which could be used as a confirmatory check, in spite of dozens of apps, programs which are all capable of doing so, many of which were field tested during the pandemic by universities.
While they might wield the ADA and HIPAA like a club, they masquerade as folks who need it.
Now, as the vaccination effort approaches a critical juncture, we see this same poisonous-allyship. To avoid personal responsibility, a handful will pretend to be spoonies. But even when they do not masquerade, the reality of their not taking the vaccine means a lower likelihood of community immunity, and they remain captors of folks who have no choice in the matter.
I wish this were the end of the part about anti-vaxx co-opting of the “unvaccinated” category, but sadly TikTok has become a strange place for anti-vaxxers to have a new trend. From the hunger games “I volunteer as tribute” phrase and salute to even using the mocking Jay whistle. This is much like the opposite of those attempting to masquerade as allies, but here instead as unvaccinated spoonies being lumped in with their “solidarity” for being unvaccinated. For Spoonies who have no other alternative to being vaccinated, or for Spoonies like myself where the vaccine is less likely to work, this is beyond insulting. We already advocate for real health problems, we don’t need this weird diversion of focus.
As spoonies we must wait for community immunity or the virus to become a minimal threat and no longer endemic to a region. Both of those are tall orders right now given those who would masquerade as allies are now effectively holding us captive, as for many of us spoonies with immune-issues will continue on as if it were still rampant, for we were the vulnerable population before the vaccine’s availability, now we could end up being even more so.
It’s also imperative we have highest possible vaccination rates for another reason: National Security.
For those uncertain about all of this, national security and disease control go hand in hand. After all, the Spanish Flu (H1N1) killed more people than any battle during World War One.
Unfortunately last month the CDC announcement of their new mask guidelines began a terrible trend. The CDC recommendation ignores evidence of transmission from vaccinated folks being similar to that of asymptomatic cases. Why is that concerning?
Asymptomatic and pre-symptomatic cases have been the dominant method of the last year for transmission. ” transmission from asymptomatic individuals was estimated to account for more than half of all transmission” This predominantly due to our minimizing interactions, use of symptom checkers like thermometers, and mostly because folks who felt ill were told to stay home and given additional sick days to accomplish this. So now, as we move about again, and the majority of folks, functionally become like asymptomatic cases, are less likely to be tested because they are vaccinated, and are less likely to feel unwell, prompting less caution regarding transmission. Public health experts have repeatedly gone out of their way over the past month to explain the necessity of these masks after vaccination, and a recent study highlights these points. And with the data that we’re seeing here, with so many folks not vaccinating, The CDC mask policy only makes unvaccinated folks more vulnerable. So to see that Cal/OSHA, Newsom and the lot of them caved again to “business leaders” AKA Big business is absolutely unconscionable for a number of reasons. And to cave in an odd way, to no longer recommend that workers, even in high-risk jobs, wear a mask is likely due to additional pressure from the recall campaign.
1. Pandemic still raging around the world, importation risks remain high, especially with new VOCs.
2. It’s not even close to eliminated here in the US, and with states like Florida abandoning important info and their COVID-19 dashboard, (despite being the likely source of new VOCs in the US due to their lax testing criteria and outright dangerous vaccine policies for travelers, and the medical tourism for vaccines) transparency is WORSE than in March 2021 when dashboards finally started working.
3. The tests still kinda suck! Due to the windows of false negatives no current test breaches about 60-80% in sensitivity aka false negative rate. The problem is the way the virus does it’s thing compared to the administration of the test on the patient timeline, some more sensitive tests exists, and saliva testing has shown to be more robust in early detection than more typical NP/OP swabs.
4. The CDC mask guidance dropped months earlier than it should have, using them as guidance to make things consistent has nothing to do with health, rather with consistent regulation showcases our Safety 3rd mentality regarding health regulation.
5. When we consider the rates of potential folks who cannot vaccinate alongside the folks who will not, these numbers make community immunity potentially our of reach, especially with continued importation of cases, which can see more clearly with VOCs. All of these decisions seem quite premature.
In situations like this, caution is the better decision, moving slowly, with available data.
Right, Rick, but how does this affect you personally?
I’m a transplant patient, who is planning my vaccination with my doc, it means waiting more than I’d like, it means seeing those around me start to engage in a slowly opening world. It means saying no to networking opportunities, potential career-boosting opportunities, and a great deal of advocacy. It means having limited interactions with friends and family even though the vast majority are vaccinated. Having close family members who are also in the same Spoonie boat, increases our vulnerability. I’ve already spent 6 years in end stage liver disease and the last year damn, I know the fear and potential pain many in the community sense or feel. Unfortunately the vaccine may not even take due to my immunosuppressant meds and in the rare event that my antibodies are detected, it is not recommended as a confirmatory test on immunity.
Thankfully, I live in a community likely to have high levels of vaccination, and have local leaders who understand the interplay between border cities and are donating vaccine supply to San Diego’s other half, Tijuana.
But while SD county only has about 19% of its population unvaccinated currently, neighboring Imperial County has about 32% of its population currently unvaccinated. You san see County by County data here.

These percentage points, combined with the reality of growing interstate travel and vacation use, means as a tourist destination, San Diego is also likely to see more importation cases from neighboring states with less regard for health and safety. So while San Diego folks are more cognizant of their health, tourists might not be.
Okay, well that was awful, is there anything that can be done? Or are we just fucked?
I mean, for those of us in the spoonie community, we know how common the latter is, but in this case there is more that can be done. While states give away money, or Xboxes, cars, or whatever else seems clever, the reality is that folks who aren’t interested aren’t likely to be swayed by a SWOT analysis. They’re likely to be influenced by their peers. Some “Maskueraders” won’t understand so easily and it may take time for them to understand the real risk and adjust their worldview. Patience and tolerance is important.
If we want to be free again in this country, in this world, we must be prepared to protect our community, our nation, and our world, by at the least getting a vaccine for COVID-19. It probably would also help if the federal and state governments could agree on a standard for ensuring vaccination, like having some kind of universal database (it exists with HHS already it’s just not connected to anything outside of a few departments) having at the very least a robust nationwide Electronic Health Record system would help in every health fight, improve mobility within systems, reduce administrative costs, streamline costs/billing and further the goals of health equity in the American population.
As someone who has been fighting to Eliminate a different Epidemic (Viral Hepatitis) It’s imperative that we talk with friends and family about being vaccinated and encourage others around us to be honest and take the vaccine when they can.
In the meantime, please wear a mask when around others in close quarters, or in mass gatherings/mass transit, and if you aren’t yet vaccinated and can get it, please do and encourage friends and family to do the same.
TLDR:
Vaccine rates won’t go down unless we talk to our friends, family and neighbors and make sure everyone who can vaccinate does. The CDC Mask policy makes the pre-emptive reopening potentially worse, and worse for unvaccinated folks who account for nearly all cases in the US. Anti-vax folks pretending to be disabled doesn’t help anyone. Blending the category of unvaccinated conversationally benefits anti-vax movement, as they pretend to be martyrs (who don’t think they’re going to die? it’s confusing) Expanding poor health policy only further erodes what little public health trust exists in institutions. We can always hope it’ll turn out alright, but as a six time survivor of Hep C treatments, my caution regarding Epidemics is imbedded.
Johansson MA, Quandelacy TM, Kada S, et al. SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA Netw Open. 2021;4(1):e2035057. doi:10.1001/jamanetworkopen.2020.35057
La Marca, A., Capuzzo, M., Paglia, T., Roli, L., Trenti, T., & Nelson, S. M. (2020). Testing for SARS-CoV-2 (COVID-19): A systematic review and clinical guide to molecular and serological in-vitro diagnostic assays. Reproductive Biomedicine Online, 41(3), 483–499. https://doi.org/10.1016/j.rbmo.2020.06.001
Patel MD, Rosenstrom E, Ivy JS, et al. Association of Simulated COVID-19 Vaccination and Nonpharmaceutical Interventions With Infections, Hospitalizations, and Mortality. JAMA Netw Open. 2021;4(6):e2110782. doi:10.1001/jamanetworkopen.2021.10782







