Well, this was supposed to be about the economy, but that’ll come later.
While each of these *can* be read independently, it’s best when read together: First Article, and Second Article.
With the release of the C.D.C.’s new updated Mask recommendations and the reactions from cities and the W.H.O. over the past few weeks, it’s about time we actually see a scientific approach to mask guidance and a bit about boosters and how this all works together in your toolbox of dealing with the pandemic.
First, let’s talk about the title of the article, “Trust me, it’s raining.” We’re diving into the importance of public trust in agencies and how, unfortunately, science isn’t always the driver of a decision as much as we’d like to think it is. Because in May, the C.D.C. and the Biden Administration’s messaging was akin to pissing on our shoes and telling us it was raining. Unfortunately for us, when it rains, it pours.
It’s also meant as an analogy we’ll talk about later when it comes to preparing the tools in your intervention toolbox, how they layer, and how to think about daily covid protection, more like weather, or well, rain.
A few weeks ago, amid the new mask rules, the C.D.C. also acknowledged that transmission has been occurring among the vaccinated population. For some reason, this tidbit seems to be very misleading among folks, from advancing concerns about the effectiveness of the vaccine vs. the new fears of Delta/V.O.C.s… but this reality makes their previous guidance seem suspect.
Because in terms of the data and Literature at the time, it was. It was a political decision to not simply repeal the mask guidance prematurely, but to encourage abandonment of interventions once vaccinated… Public Health experts have been beside themselves this entire time. When vaccination rates scuttled, the hope that F.O.M.O. would encourage folks to get vaccinated not only fell flat but helped encourage cases to spread.
In my previous articles, I’ve explained the reality reservoirs play when large groups of folks refuse to abide by interventions designed to decrease the incidence of COVID19. Those being mask-wearing, physical distancing, increased hygiene/handwashing, and of course vaccination when medically reasonable.
Before we dive into why the new C.D.C. guidance makes sense and how we should incorporate the new “covid weather map” into our daily lives, let’s talk about that last intervention.
The vaccines are solid, they work well, and are unlikely to require a booster any time soon. In November/December, that may change. (although the WHO, taking a political knee and saying please stall until September for boosters to the developed countries pushing boosters) It’s important that the target for vaccination should be the most folks getting fully vaccinated before boosters become common in developed countries, if we want to eliminate the global recurrence of new VOCS at the rapid pace we’ve seen. “In the context of ongoing global vaccine supply constraints, administration of booster doses will exacerbate inequities by driving up demand and consuming scarce supply while priority populations in some countries, or subnational settings, have not yet received a primary vaccination series. The focus for the time being remains on increasing global vaccination coverage with the primary series (either one or two doses for current EUL vaccines).” as stated by the W.H.O.
That being said, if our current V.O.C. trend continues, sometime next year, a booster would likely help the more vulnerable populations and may be indicated for everyone should the virus find new footholds. The science behind boosters is sound, and the data reflects the protective quality of the vaccine. We have always known that the vaccine likely protects to a certain degree against infection but that it does not always prevent transmission.

Our current messaging on the pandemic is, well… bad. It’s exclusive, shame-inducing, and it’s basically the same strategy we always use: shame, aka peer pressure. Does it work? To a degree, but it has a weak range of effectiveness, it always has; Project D.A.R.E. is ineffective(West, 2004). If you suspect it works, I D.A.R.E. you to consider other similar strategies met with bucking shame and tribalism like the “War on Drugs” and, well, Condom use.
When we hear messaging on vaccination, it blames the unvaxxed for all the problems we’re experiencing, as if they are the source of the new problems. Which while partially accurate regarding V.O.C.s, it’s also important to remember that this is a virus. And no one is at fault here.
Leaders who use their platform to spread misinformation or disincentivize folks from taking the vaccine or following other interventions do bear a degree of blame for which society should interpret sooner rather than later.
It’s important to consider the US CDC messaging isn’t happening in a vacuum, it’s happening in a world where 20-30% of the population cannot afford the vaccine under the current conditions, and somewhere around 20% are struggling to access for a lot of different reasons, but mostly to do with cost or the convenient opportunity to commit genocide with less potential blame. Currently, about 30.4% of the world is at least partially vaccinated, only 15.8 are fully vaccinated, and the U.S. just passed the 50% mark on fully vaccinated (two weeks after the last jab.) Pandemic is global, an important reminder here is that V.O.C.s have come from other countries, as well as being amplified in the U.S. Importation of cases will constantly be an issue when states like Florida are a hot-bed for the circumstance due likely in part to DeSantis political ambitions overweighing safety for the American people. Between instituting a mask-less requirement for all Florida schools and threatening district leadership with pay cuts if they try anything(and now that pushback), I don’t think we’ve yet seen the worst of his policies, as they continue to ignore evidence and enjoy cherry-picking data.
The U.S. C.D.C. messaging creates a specific narrative that does not help to eliminate the pandemic.
The current C.D.C. messaging focuses on pressuring the unvaccinated as the cause of V.O.C.S. and the reason for our current surges, which is a half-truth. The vaccinated, are, unfortunately, also spreading SARS-CoV-2, as much, if not MORE, than unvaccinated due to their larger numbers and similar lack of adherence to interventions; the difference is in how far that spread goes. The evidence regarding vaccinated folks carrying the virus has been known for some time; the initial SARS-CoV-2 virus had been shown to be transmissible among vaccinated, but far less than typical. We also suspected V.O.C.S. might change the game up. On March 10th, J.A.M.A. Viewpoint from the C.D.C. “A growing body of evidence suggests that fully vaccinated people are less likely to have asymptomatic infection and potentially less likely to transmit SARS-CoV-2 to others. However, further investigation is ongoing.” (Christie, 2021)
“The risks of SARS-CoV-2 infection in fully vaccinated people cannot be completely eliminated as long as there is continued community transmission of the virus. Vaccinated people could potentially still get COVID-19 and spread it to others. However, the benefits of relaxing some measures, such as quarantine requirements, and reducing social isolation may outweigh the residual risk of fully vaccinated people becoming ill with COVID-19 or transmitting the virus to others.” (Christie, 2021)
This is from a paper the C.D.C. director co-authored; the tone was already being set for the shift in messaging; however, what’s certain, was that we should not discourage interventions but relax measures according to regional outbreaks. California’s tier system successfully allowed counties to better control their circumstances; the lessons learned would have been easily translated, as they more recently have been in the new C.D.C. guidance.

But…following the strange shift to ENCOURAGING vaccinated folks to resume all activities without consideration for interventions was at the very least reckless. The medical blog site The Conversation echoed how most Public Health folks felt about this strange messaging. “Vaccines can be great at preventing you from getting sick, while at the same time not necessarily stopping you from getting infected or spreading the germ.” (Mishra, 2021)
We knew caution was essential to maintain because many suspected immune escape and viruses to continue to create potentially new V.O.C.s when the subvariants affect one another. We knew immune escape was a potential problem, we suspected increased transmissibility of new V.O.C.s, and yet not until weeks after Biden’s celebration regarding successfully not reaching 70% by July 4th and more information coming out about Delta did the messaging shift.
For those of you who are interested in high-value content regarding accurate information about COVID-19, might I suggest https://www.covidhealth.com/ and https://www.unbiasedscipod.com/ They put out lots of well-designed graphics and sharables like the one below.

Important regarding the Delta V.O.C., The increased transmissibility is roughly twice as potent as the original strain, increasing viral load early on by as much as a thousand times higher. This not only indicates significantly more pre-symptomatic transmission, but importantly it improves the sensitivity of our PCR tests. Previously, PCR tests had a false negative rate which decreased to near nil close to day 5, but due to the increased viral load, Delta is detectable earlier than the original strain. Overall potentially improving test sensitivity by upwards of 10-15% due to the smaller windows of false negatives.
People were grossly unaware of the reality of the problem partly because the news doesn’t understand public health. Occasionally the NYT has been helpful regarding their data; however, their interpretations, opinions, and articles vary immensely based on its author.
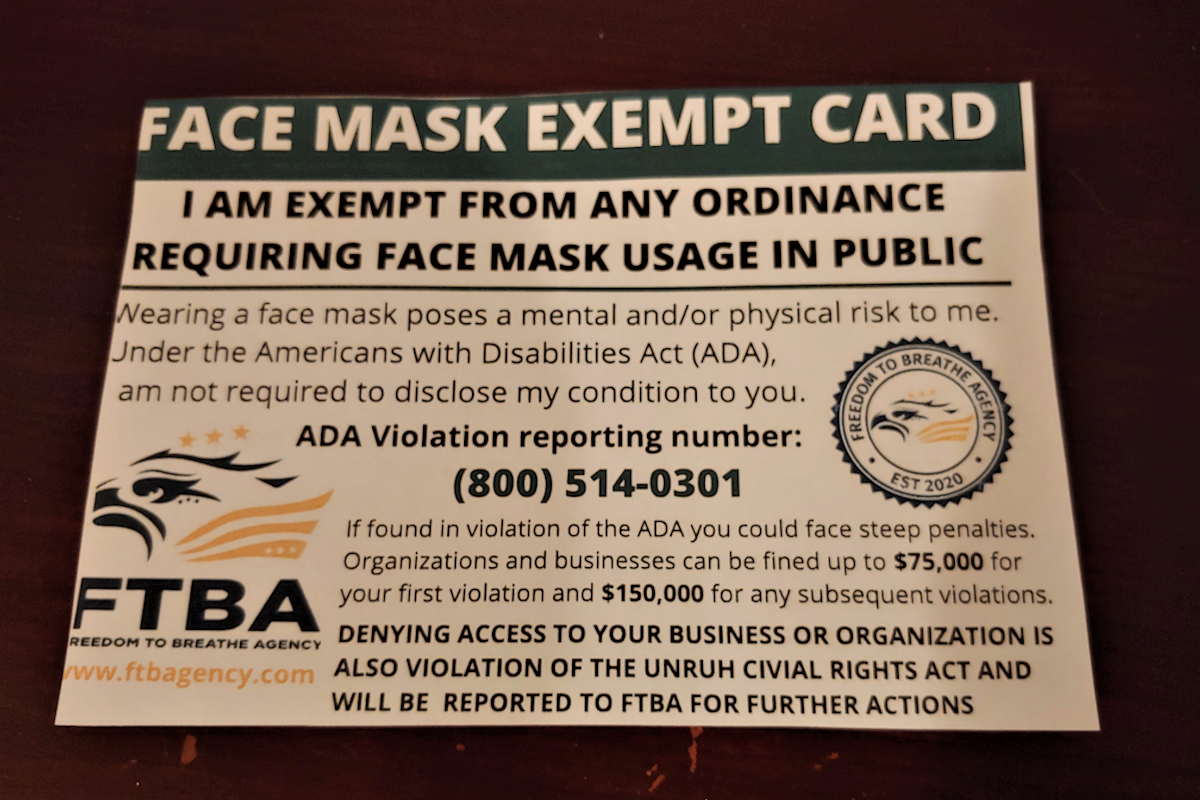
This discourse was confusing for the general public because of media trash like this.
Made more confusing by choices like this from the C.D.C.: As explained in my previous article, the C.D.C. isn’t really looking for breakthrough cases, although the states are recording data on their own. Given the political climate, this *seems* not well thought through. It’s also important to note that breakthrough cases are defined by two weeks following vaccination, which puts partially vaccinated folks into the general lump. DEBLASIO, DID YOU READ THAT? Why the Capslock? Because the Mayor of New York City’s strange vaccine I.D. requirements only need one dose to count and may repeat the Springsteen debacle of vaccine nationalism, because what vaccinations count? L.A. reinstituted a mask requirement, which is…well…easier, more inclusive, and pisses off people who don’t want cloth on their face. The LA requirement also has no teeth, so most folks will and have likely ignored it to a degree, which we’ve been seeing alongside growing tourism likely importing cases.
But now the C.D.C. finally is on board with an actual solution, and of course, folks are doubting the agency…again. Do they deserve the doubt? Yeah, I’d say they tarnished the trust with the U.S., now multiple times over masks, so this was an epic fail on the part of the C.D.C. to do this, in this fashion.
But now that we do have reasonable guidance, let’s talk about how we should live with this pandemic.
We’ll get into the nitty-gritty of just why the C.D.C. messaging is so bad after this analogy.

IT’S RAINING, MEN.
However you consider the Coronavirus/SARS-CoV-2/COVID-19/’Rona Pandemic, its essential to consider how a public health body should explain preparation for everyday folks.
We should think of SARS-CoV-2 like we do precipitation. Now, with better testing, better maps, integrated map tools into Google Maps, this type of analogy can make a lot more sense.
First, we have to look locally because that’s where the problem lies. A Pandemic in this sense is considered by its millions of regional outbreaks. So we can think of it as a massive Global super-Hurricane capable of producing all weather phenomenon.
Does it sound potentially terrifying? It should. Our toolbox of protection against rain may be raincoats, umbrellas, boots, maybe a towel by the door. For snow, we might need a snow shovel, salt, thicker coats, snow boots, etc.. We prepare for a pandemic in the same fashion, it’s just a little harder for some folks to initially see this because it’s a generally invisible threat.
The prevention toolboxes listed above are for an individual, and there are more for the community, and the State, should the weather become too burdensome on the individual. There are also toolboxes for response, maintenance/long term, and importantly for the future, meta-analysis, but let’s focus on what you can do, and maybe a bit about what some stuff around you can do.
These are the tools in our toolbox for an individual by importance:
1. Getting the Vaccine, in terms of rain( SAR-Cov-2), It’s like having a scotch guard bubble, one’s feet might get wet, and the bubble gets scratched up as it encounters things like hail(V.O.C.s).
2. Wearing a mask is like an umbrella, so if any water does get in, one is still dry to a degree, but one’s feet still get wet. (benefit is an umbrella can reduce the rain for others nearby, but don’t share masks)
3. Interactions are a combination of physical distancing and time. These are the boots, and how they’re used determines what type of boots they are and to what they’re resistant. The less time an interaction requires, the stronger those boots are, the greater the distance the interaction requires, the more protective those boots are. E.G., If an Interaction takes 15 minutes, and someone can keep a distance of 6-8 feet, that interaction previously ran a low risk but now runs a low but higher risk with Delta. It would be like wearing boots with worn soles a small hole in moderate rain; socks likely will get wet the longer the stay, and with random hail(V.O.C.s), it’s making the water splash about getting the bottoms of pants wet.
4. Airflow, often this can be considered Inside Vs. Outside. There are lots of ways to improve or increase airflow, opening windows, using air purifiers, increasing the cubic footage (typically heightening a room), adding negative pressure or exhaust fans. Each of them, like every intervention, mentioned, layers to add protection against SARS-CoV-2 and its V.O.C.S.
5. Hygiene isn’t just washing your hands. In this case, it’s cleaning your hands after you interact with things in new buildings or commonly touched items outside. It’s avoiding touching the face, nose, and eyes while not in the home. It’s the analysis of our washing routines to make sure we enter our homes clean, which can mean taking a shower after a long day at work if work is in a public or shared space with lots of people. Hygiene also reduces our risk of getting multiple illnesses. Some folks might wear lycra gloves to avoid constant handwashing, but they should rotate through sets as they go from location to location.
6. What? There are more tools?! What else can we do? Vote for political candidates who aren’t actively telling others not to or disable their ability to do any of the above. Really. This is by no means an endorsement of any political group; it’s just common-sense Public Health. Leaders who broadcast and elect to enact policy making an outbreak easier are objectively a bad choice during a pandemic.
7. Hah! There’s even another one, because the Internet. Correct misinformation to the best of your ability, even your own. The Scientific Literature is constantly growing and correcting itself, and when agencies interpret this, once an Administration is involved, it has to consider what obligations or national temperament may require. This is part of why C.D.C. Director Walensky removed the mask requirement because it would release tension regarding intervention compliance, giving a break, for what she would have likely suspected, was a wave coming in the Fall. The likely additional guidance by the White House to disregard all interventions once vaccinated was likely weighed with the unknown of Delta. The Literature expanding to include the significantly higher transmissibility put pressure on the C.D.C. to install the current system, one which always should have been the guidance. But Literature doesn’t guide every government decision; there are a lot of data to consider, including compliance with interventions. So government agencies have a degree of fallibility here. But it’s crucial that when we correct misinformation, we shouldn’t be a dick about it, speak honestly, but withhold that new Government Encouraged Outrage.
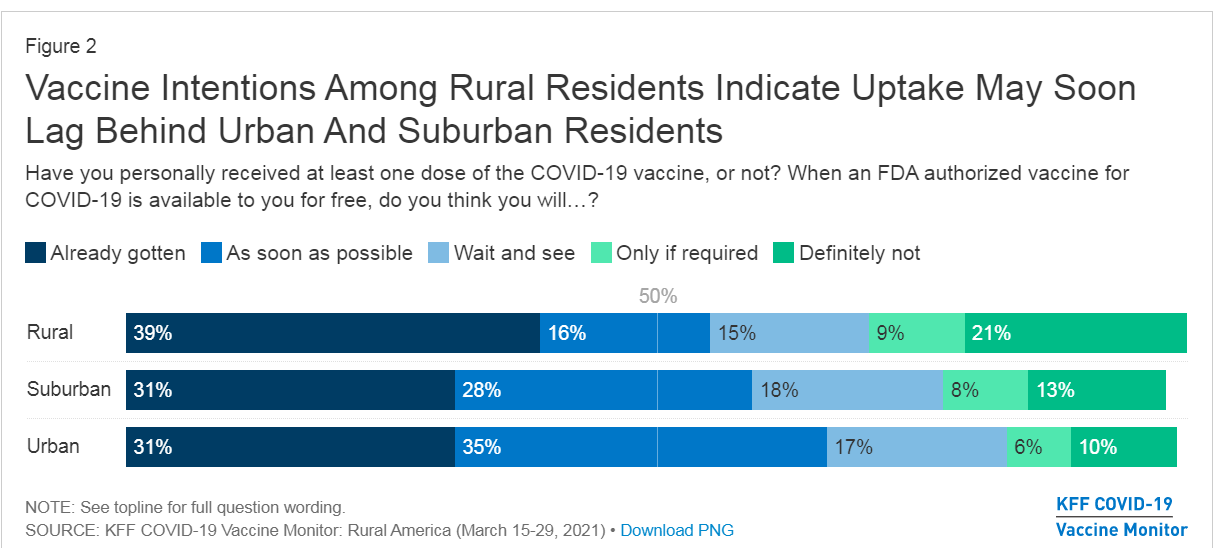
For a moment, to see how the messaging is doing to improve vaccinations, let’s return to the K.F.F. Vaccine Monitor to see what stalwarts likely remain, besides those of us with chronic conditions who require the timing to figure out when to vaccinate or who simply cannot given the current guidance with their doctor. We should assume that the vast majority of them would likely answer “Wait and See” and a few as “Definitely Not”, but not enough to break 4-5% and 1-2% respectively of the whole. So about 20% of Americans still leaves many folks who aren’t interested in vaccine-induced immunity for whatever reason.

But the most compelling thing from this month’s K.F.F. Vaccine Monitor was this unsurprising comparison “News Of Coronavirus Variants Has Caused Some Adults To Change Behavior, Two In Ten Unvaccinated Adults Say It Has Made The More Likely To Get Vaccinated” vs “A Majority Of Vaccinated Adults Say News About The Possibility Of A Booster For The COVID-19 Vaccine Hasn’t Caused Them To Worry About COVID-19 Protection, Black And Hispanic Adults Slightly More Concerned.”
These data illuminate that the white house messaging DARING folks to get vaccinated to avoid creating V.O.C.S. and blaming them for the new surges aren’t having the desired effect of increasing demand for vaccination.
So it’s time to consider what’s next. The increased vaccine employer requirements are absolutely squeezing the “only if required” crowd down to zero. Still, the remaining potentially 15% by the end of this year who will be Choice Unvaccinated might be enough to continue this nonsense for another year yet, instead of going from mitigation to control like in New Zealand or Taiwan.
How do we convince the stalwarts? Talking to them helps, but only when it’s productive and informed.
A big thing, though, is honestly, ignore the big fluffing. The thought-leaders encouraging anti-vax thrive on being the underdog and defending their position, don’t give them clicks, just brush it off like the nonsense it is, and also don’t feed the hating on them, ya know, like the U.S. C.D.C. messaging inadvertently does.
It’s important that we all agree on something here, though, that no one deserves COVID-19. Leaders do bear some responsibility; however, that doesn’t mean someone deserves a life-threatening condition that could result in a chronic illness or death. If we want to get through this pandemic, the only way we can is together.
By considering the Interventions relative to the danger around us, much like we do with weather every day, we can best take caution to protect ourselves and our communities. We may not always need to wear a mask all the time, but when the risk is high, we should take as many precautions as possible and use as many tools as we can carry.
Get Vaccinated when/if you can. Wear a Mask indoors, in crowds, and in mass transit. Also, consider the other tools as the situation demands.
References
Christie A, Mbaeyi SA, Walensky RP. C.D.C. Interim Recommendations for Fully Vaccinated People: An Important First Step. J.A.M.A. 2021;325(15):1501–1502. doi:10.1001/jama.2021.4367
Lazarevic I, Pravica V, Miljanovic D, Cupic M. Immune Evasion of SARS-CoV-2 Emerging Variants: What Have We Learnt So Far? Viruses. 2021; 13(7):1192. https://doi.org/10.3390/v13071192
Levine-Tiefenbrun, M., Yelin, I., Katz, R. et al. Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine. Nat Med 27, 790–792 (2021). https://doi.org/10.1038/s41591-021-01316-7
Mishra, S. (2021, July 29th). Can people vaccinated against Covid-19 still spread the coronavirus? The Conversation. https://theconversation.com/can-people-vaccinated-against-covid-19-still-spread-the-coronavirus-161166.
West, S. L., & O’Neal, K. K. (2004). Project D.A.R.E. outcome effectiveness revisited. American journal of public health, 94(6), 1027–1029. https://doi.org/10.2105/ajph.94.6.1027