But across all of my online dating profiles I will openly disclose that I have HCV along with pertinent information.
My virtual identities which I once held separate I’m going to link.
I don’t really know what will happen.
I don’t know how people will take it.
But we’ve all got our shit.
In addition to doing the ongoing dating series…
Next month The Five will be available to read in it’s first iteration in six parts.
It is an introspective look at the previous treatments’ failure and how to fail best.
(like Astronaut Chris Hadfield says “Visual Failings, not Defeat” )
As May is coming up, I wanted to highlight the amazing changes that have happened in the past year when it comes to treatments and the bright future there is for those with Hepatitis C.
Of the daunting challenges to overcome, awareness can help address one of the largest ones. The fact that the majority of those who have the illness will go unaware until they begin showing symptoms and by then permanent damage can already be done.
It’s easy to understand why this can be a terrible idea, but considering 1 in 20 Google searches are medical related it’s not hard to understand why it was done.
For those of you not hip web-lingo, it’s a scraper. Scrapers copy content and aggregate data onto one platform, typically a website, however recently apps have become fantastic at using scrapers.
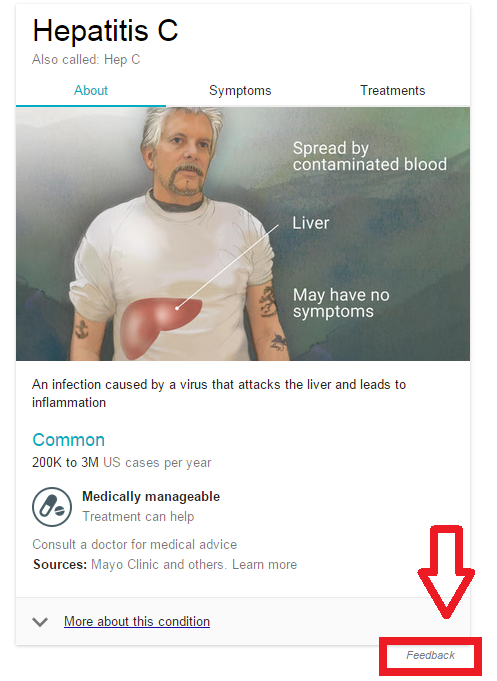
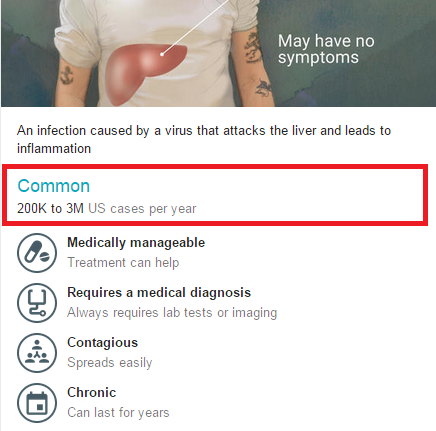
Let’s look at the 4/12/15 Google high-quality image medical data for Hep C.
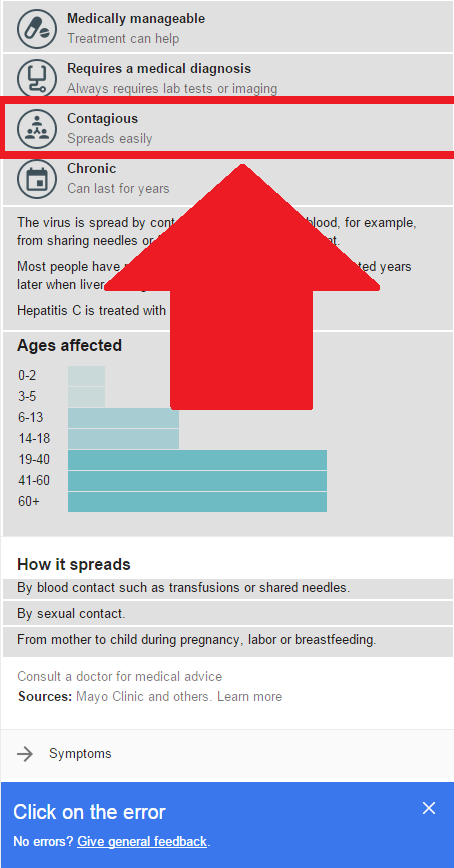
This has recently changed from sexual contact to spreads easily.
I can see a glaring issue without having to go much further. Under contagious its top listing says that it’s Mainly spread by sexual contact.
The main methods of transmission are in order: Intravenous Drug Use, Transfusion (in the USA prior to 1992, in Canada prior to 1990), and needle stick/Health care worker exposure.
This is the principle problem with scrapers. Even it grabs the data properly, Sexual intercourse using has the longest section when describing the transmission methods…why?
Because there is a lot of controversy around it. The most recent poll was done by the CDC in 2010, and the questions that were asked, were fairly direct. Even in other polls that have come out through the years, this issue always comes up: The biggest section of the Hep C population consists of Intravenous, mostly illegal, drug users. It’s far less damning for someone to claim to have received it sexually than via drug use.
When studies have polled HCV patients directly, usually through a doctor, they find slightly better information, which is why we have such an interesting spread of information. They also have been examining the virus, to see how likely these claims could be. E.G. looking at the life of the virus outside the body, looking at how the HCV RNA in sperm is typically inert or non-existent. (it’s around 9% of the HCV infected male population that have it, and less than 20% of that 9% excrete enough for it to potentially be transferred) The less likely means of transmission as in order: Vertical Transfer: Mother to Child (it does not go father to child), Personal items (nail clippers, razors, etc..), Sexually can even further be broken down: Rough unprotected anal intercourse, rough unprotected vaginal intercourse, unprotected intercourse/rough intercourse. It is not simply by means of sexual contact, which is a much larger category.
Okay Google, now…let’s talk about how we correct this problem. There is a feedback button at the bottom for correcting mistakes.
But this is also terrible, because most of the time people who Google ailments and diseases are usually anything but experts. So the idea that an under/uninformed user is going to be able to use that feature is silly, at best. In fact, many who use this method, may reinforce what Google says by repeating their new-found knowledge to others who are under/uninformed.
The feedback method is used a lot by Wikipedia. And the correction method works for Wikipedia because often times authors/experts will correct the information using verifiable credentials. But even still, Wikipedia’s accuracy is at the mercy of its users.
The other issue with this new presentation of information is the listing of sources. Google is borrowing the credibility of the top websites in its scraper. The Sources listing as “Mayo Clinic and others” uses a recognizable name to help a user view this information as accurate. Additionally there is no list, of what these sources area.
Ethically it should list sources, as “Sources” and not disclose any of them until the user checks the sources themselves.
While yes Google consulted with the Mayo Clinic, clearly not for that medical data, which is what makes this tool so useful. Not only would it allow Google a better idea as to how many of their users trust this quick medical information, but it would also allow Google to randomize the presentation of sources to encourage users to verify the medical information.
Why? Because if you see Mayo Clinic, 9GAG, WebMD and Top Ten medical facts about DISEASE YOU GOOGLED listed as sources, chances are you’ll look at the info with more scrutiny. Since then, Google has changed the main transmission method to “Spreads Easily.” Which, as a blood-born pathogen is far from the truth. Please Google Hep C, and help correct it. Also if you’re a medical professional, please help correct the information you know to be false. And please ask your Doc/Specialist(s) to help correct false information as well.
While there is a lot of medical information on the web at your fingertips, always tread with caution. Incorrect information, or half-cocked information should never be used for diagnosis. The internet can provide you with the questions you need to ask, the help of communities, and other resources to get help.
Misinformation for medical information is potentially deadly, and after all the internet is mostly a series of tubes.
Step 1: select the feedback button at the bottom of the app.
Once you’ve selected the feed back button it’s time for Step 2.
Step 2: select the “contagious” category highlighted above.
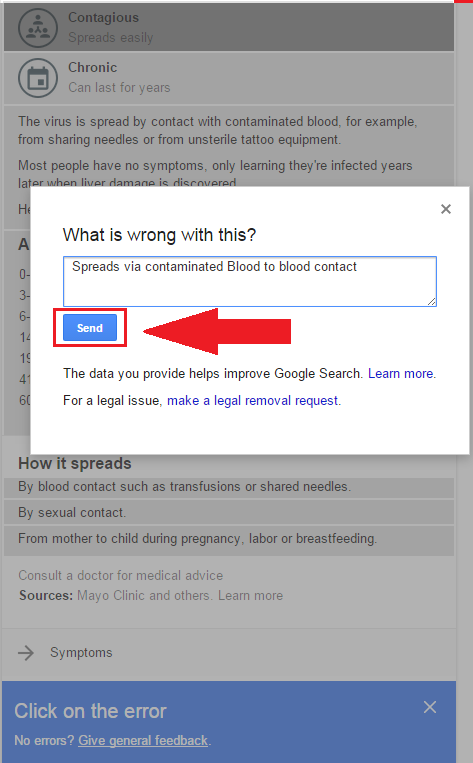
Step 3: Once you select that category a “what’s wrong with this?” will prompt. Please enter “Spreads via contaminated blood to blood contact”
Step 4: Select/click send!
Once you’ve clicked send, this message will display confirming you submission!
And Voila! within a few seconds you’ve just helped correct a major problem! There are two more sectors with the same issue however… there’s still more incorrect info.
So please put: “About 22k new cases per year, 3.2 million Chronically infected persons in the US.”
Under Treatments tab,
The Prescription category :
“Simeprevir rarely used in US. Should be sofosbuvir/ledipasvir (Harvoni) or ombitasvir/paritaprevir/ritonavir + dasabuvir (Viekira Pak), with or without ribavirin”
With the CND underway and news about ACA/Obamacare, A lot of healthcare related issues are on the table, nationally and internationally. If you’re interested in keeping tabs on what’s going on with drugs/pharma and all things narcotic internationally i highly suggest checking out the blog, or if you want something easier to digest check out the twitter hashtag #CND2015.
But as for the ACA/Obamacare… Let’s talk Healthcare Insurance.
Healthcare basics: Healthcare as an employee (which is the most common way about it in the united states).
Insurance and compensation are part of the bargaining agreement between you and your employer when you start working for them.
Insurance is a weird thing, but ultimately the employer is giving you a discounted insurance plan in lieu of other financial compensation. There are some companies that will pay you to opt out of their insurance, because it’s cheaper for them as long as they meet their units needed for group discount.
So when you get handed a dozen options from your HR department come fall, I’m sure you’ve noticed a few plans are ridiculously expensive. In some circumstances companies have executive plans which cover more than the options you were given.
Your pay-grade usually determines the allowance you get to buy a healthcare plan. It would be prudent to know that the ACA is the first real legislation to present a progressive tax system that extends to this compensation.
Why should you give two shits about all of this? Understanding benefits negotiations is as essential as negotiating your wages. Since it’s such an information disparity, most potential employees do not know what they’re going to get until they’re hired. It’s always good to know what insurance plans are offered by a company and how they compare to other options.
It’s also often the case that you may find that your doctor is no longer covered when you switch employers, even if it looks like the same plan. That’s because Healthcare plans usually have a list of doctors within their program. There are some medical groups that have associated healthcare insurance to alleviate this issue, and in a sense compete over your care without your say.
The necessity of Insurance.
Health insurance since the early 80s has been a rapidly growing part of paying for a hospital bill. Insurance is and always will be an all or nothing deal. Whenever Insurance becomes part of a marketplace it sets group rates and raises prices for those without insurance. This alongside Pharma patents, costs of medical equipment, and a disturbingly small pool of workers has helped to create some of the unusually high medical costs we see today.
Because healthcare insurance has become part of an employee’s compensation, healthcare is more often the primary means of payment for most medical groups. The employers bargain with insurance companies for rates and plans, those insurance plans present proposals to medical groups. For the most part the conversation regarding what you pay for healthcare is never up to your needs, and the services you choose from are what the companies have agreed upon. Limiting your choices as a healthcare consumer.
Exchanges allow for consumers to pick plans they would have otherwise never seen. Their major limit is their geographic region. If you’ve used Covered Ca, Healthcare.gov or even a private exchange you’ve seen how much better many of those options can be.
Payment without insurance is always higher, and if you’re savvy you might be able to negotiate a payment plan with the hospital’s billing and/or finical assistance dept.
But regardless you’ll pay more. This is one of the fundamental problems the ACA attempts to alleviate. The reality that if you’re employer doesn’t give you benefits(usually not fulltime), underemployed, or hanging income-wise out between 17k and 40k per year: you simply go without insurance, and risk falling into serious debt/health problems when something bad happens health-wise.
It also alleviates the issue of employer based competition by opening up the markets to consumers via exchanges.
In our modern society, being so close quarters and risking illness/injury daily, it is necessary. So… I guess I should get to why I’m on this subject right now. Well, the reason I’m talking about this is because this last week the Congressional Budget Office announced its projections for 2015. The ACA (Obamacare) has a very interesting track record.
While there are a lot of disagreements as to why these changes are occurring and how it affects us, esp. with King V Burwell presently in the Supreme Court. To insure our health as a nation, the subsidy is an important factor alongside the exchange.
What’s noted here are some relevant facts: Affordable Care Act(Obamacare) will have lower projections in terms of cost and number of people covered using the exchange.
And these are the real changes in 2015
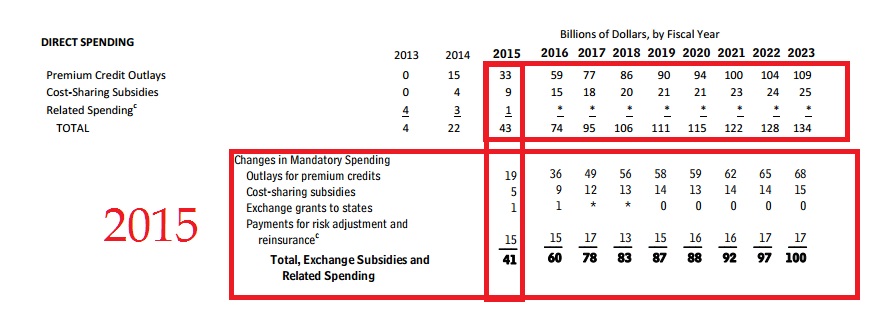
In order to better illustrate the exact changes, I’ve made some comparison charts using the data from the Congressional Budget Office:
Table 1
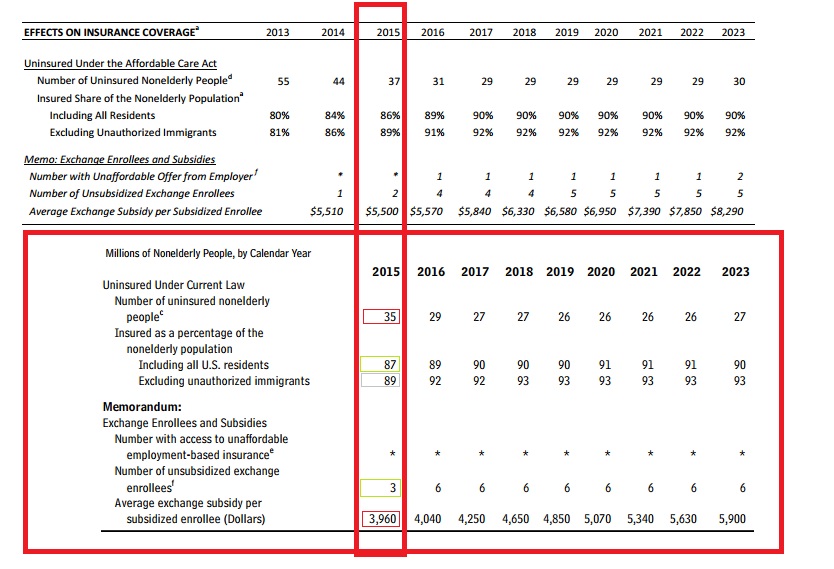
Here’s the neat bit of all of this, since we’re halfway between a census it’s hard to have spot on population projections, but 6 million less non-elderly people than projected is a doozy. With projections the relationships between the numbers are important. The goal of the ACA was the lower the number of uninsured. Expanded healthcare to 26 under parents plan, lower of full-time work requirements, the subsidy/exchange program, and 400% poverty wage definitions helped this relationship are all parts of the ACA that help accomplish this.
Table 2
As Table 2 illustrates there is a drop of enrollees in exchanges and Medicaid. There is also an overall shrinkage of about three million people. Two things will change these numbers over time: As states allow their constituents to use exchanges, and as signing up through an exchange becomes more user-friendly we’ll see better reflections.
While politicians bark at each other, the key to keep in mind is the relationship between the numbers.
Those signing up for exchanges vs. less uninsured is nearly the same (13/20) 65% for 2013 projections while (11/17) about 64.471% for real 2015.
This relationship implies the success/failure of the exchanges as it relates to helping those who are without insurance, in comparison to projected numbers. The numbers are not much different..
Those benefiting from the ACA’s exchange and expanded Medicaid definitions also are very similar from 2013 projections (20/24) about 83.33% while 2015 real (17/21) about 80.95%.
This relationship implies the success/failure of the ACA’s exchange program and expanded Medicaid definitions, in comparison to its projected numbers. Within one year, a little more than 80% of the United States’ uninsured population gained insurance they otherwise wouldn’t have. It’s actually more than that, but the table 6 has more data to better reflect that question. This number is a close expectation of the direct effect of the program.
Table 3
These are the big numbers most people are talking about regarding the success of the ACA/Obamacare. that overall Costs are down. Woohoo! Just Kidding. It’s really not that big a deal, spending allocations are very hard to project without a few years of historical comparisons.
Table 4
Again, Table 4’s numbers reflect the overall shrinkage in projections for 2015 vs. actual. This is just a more in depth table of where that exchange enrollment from table 1 looks like. What’s important to note is that more people signed up who are unsubsidized than expected. Realistically this implies a success of offering exchanges to consumers, rather than the importance of the subsidy. This implies that states not allowing exchanges (state by state means that it’s plans better reflect their constituents) penalize their residents by lack of consumer choice at the very least.
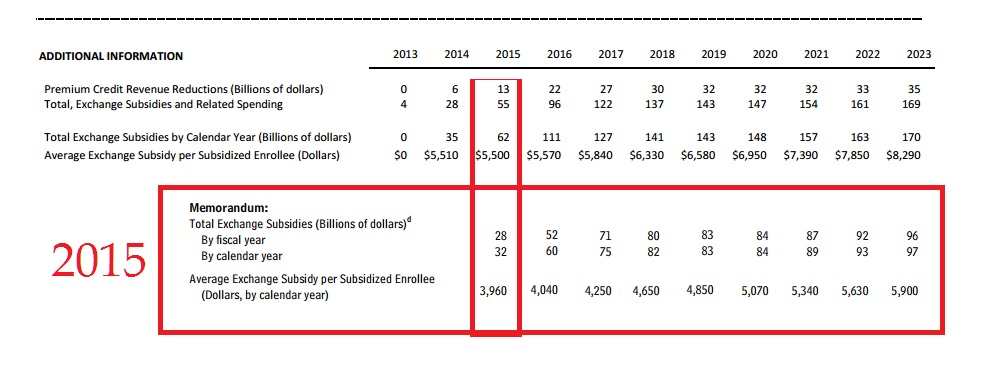
Table 5
If you want to count a huge success of comparative projections… it’s right here: Spending per enrollee dropped, by $1,540 per year.
It cost 30 billion dollars less than expected for its subsidies. The huge drop in per price enrollee eliminates the 3 million less enrolled(than projected) as a being a major factor in that cost reduction. Which means that as the program grows, it will cost less than expected overall.
Table 6
Table 6 shows clearly and definitively that an overwhelming majority of uninsured population now has coverage. Success is hard define though, because yes, this is a goal of the ACA, however, it’s still missing a lot of people.
The trouble with a lot of this is that there were no clear “Success” guidelines given to the general public. What a politician says to the people, and how s/he defines a metric are often different. The more flowery language gives a program lots of room to fail or succeed. But as we’ve all seen, it also opens the door for serious slanted criticism, and interpretation. So instead of speculate what the actual goals of the program were, let’s look at the impact.
Warning here be minor economic analysis:
There are two million less uninsured than projected, and one million more enrollees did not use subsidies. These factors helped keep the percentages about the same as projected. As the number of people who are insured rise, it’s going to affect what those without it are paying nationwide. By using healthcare insurance, their rates are already bargained and while they are the patient they’re not entirely the consumer at the hospital.
e.g. If a thousand people pay rates, each one of them has a voice. Two hundred of them band together to bargain collectively under the name of insurance. Collective bargaining allows groups within that thousand people to command better rates by demanding a certain price. Because the hospital wants a guarantee that it can get those two hundred people lower rates can be negotiated. This in turn can push prices higher for everyone else. When the bargaining groups make up a good chunk of the market it can help push costs even higher. Especially since, the bargaining groups are usually stuck with an exclusivity deal with that hospital.
As more groups arrive and become more of the market, those who aren’t in the groups can face significantly higher rates than they used to. Eventually there is a point at which the groups will command the market together, at this time they will be able to break exclusivity either the group will seek more hospitals to grow its membership and/or because the hospital will try to compete with other hospitals. There’s not really a set point where this can happen, the number of competing hospitals, and area employers can play a large factor in the use and availability of buyers respectively.
The impact of the exchange will allow for more insurers to create more diverse products. It has and will continue to compete among pools of people who before were part of bargaining groups (usually through an employer) or simply individuals who didn’t have access to the insurance(be their rationale to go without: financial motivation, lack of knowledge or what have you).
What the ACA/Obamacare has created is a marketplace for competition, and as the percentage of insured Americans increases so will the prices for those without it, which will encourage them to be part of it.
Referring back to table 6, there is one area where the ACA/Obamacare is assuredly a success. It’s price per enrollee is much less than expected. Keep in mind that the projections for the uninsured population being 2 million less does factor into that, but it’s not enough to cause a drop that large.
The ACA/Obamacare has helped millions of people have access to healthcare, and it’s not as expensive as it was projected. In terms of efficacy and impact this isn’t government cheese, it’s a marketplace where you can afford to choose a health insurance program.
While missing a dose Harvoni had no ill side effects, I can’t say the same for accidentally doubling up. Last weekend I did just that, the side effects were quick and unpleasant. I was unsure as to whether or not I had taken my pill, and while I know that “if unsure if you’ve taken your RX, don’t” is the general rule, I was mostly certain I hadn’t taken it. So an hour following the first pill, I took my second. I didn’t notice how thirsty I was until the pain began two hours in. I’m prepared for hepatic encephalopathy, ascities, jaundice, fatigue, etc… but what I can find few solutions for is the arthritic mimicry. Joint pain from time to time is one thing, but this infects every subtle movement jarringly pushing me to a slightly less uncomfortable position.
It’s not uncommon for the symptoms to express without other signs of HCV infection. I am lucky in the sense that i find myself with many of it’s symptoms, because without such challenges i may not have known of my affliction as early as i did.
Every joint in my body ached, it hurt to open a door handle. I hadn’t felt this kind of exhaustion and pain in some time. I had one solution in front of me, to wait and see. And so I slept the majority of the next few days. Drinking as much water as I could in hopes to combat my skin’s growing inelasticity. As the days passed, the extra pill’s effects began wearing off.
The RA mimicry that popped up has yet to fully fade, but at this point it’s just the state of my liver.
Nothing happened last week, which in a sense made it an exciting week.
Not because the extra pill had less ill effect than I had anticipated, but rather because of a phone call.
The week prior I had my blood drawn. I had hope that my numbers would show progress. The last few tests had shown overall that my liver function was improving, my numbers were returning to a normal state. And by normal, I mean like everybody else normal. I was constantly surprised at how well my liver function tests were going.
So now we’re here. Rather, we’re back here.
Six months ago. I was able to zero out for the first time, however when the second draw came, there was a discrepancy between the tests. Within a month of finishing my 12 week Sovaldi Olysio treatment I found myself with rapidly elevating bilirubin. Which was only further complicated by a C. Diff infection from some diner food I’d eaten for lunch. A week’s long stay and a potential transfer to the hospital for transplant were real possibilities.
I say this with an uneasy stomach spinning from caution, hope, fear, and unbridled glee.
My viral load is undetectable.
It’s unclear as to exactly when it happened, but it has been the case for at least a week. And with about 10 more weeks to go, things are looking well.
I will have several more tests, one at treatment’s end, another a month following, and yet another in August when I will hopefully reach SVR12.
It takes two. End treatment and SVR 12, Two more tests will show me that I have done, what has taken me ten years, to do. I began my first tests for treatment when I was nineteen, and just this month I turned twenty nine.
So far, nothing has been the best birthday gift I’ve received.
For over five years I went to one of the best hospitals in the nation. In that time I was on treatment twice, and unknowingly suffered from ascities. My specialist in that time had seen me a grand total of nineteen times. I primarily had to make appointments with his Nurse Practioner (NP) in his stead.
For those of you not familiar with NPs, NPs are nurses who’ve gone beyond what an RN can do. NPs are essentially doctors without the MD, but have a more applied and patient-related experience. An NP, however, does not necessarily know how to handle some extreme or unusual cases, nor do they have the ultimate say in a patient’s treatment. For these five years I had two different NPs, neither of whom fully investigated the scope of my issues, and when they did, the specialist was scant to provide a timely remedy. He was so hard to get an appointment with. I recall waiting three months for a time during the middle of the day, in the middle of the week, which was rarely fulfilled at the scheduled time– I often spent hours in the waiting room. This was in part due to him being the only GI allowed to treat HCV in my part of the county’s clinic.
Why was this acceptable? How could a hospital be so reliant on one man for their Gastro-Intestinal department? They built a system that favored surgery. I would learn his unavailability was in part because he did operations on Fridays and Mondays. Their GIs rotate surgery within the county and because of this can handle overloads in many localities, which is amazing. However it doesn’t excuse the lack of dedication to the medical office side. It also didn’t help that he was often out of office at speaking engagements elsewhere.
I had been with another medical group before this, and their specialist availability was equally horrid. This is why I suspected it was the norm. It would turn out the other group had a similar issue, only their doctors worked for multiple contracts at hospitals…literally next door. And they refused to see the need to hire more.
These two groups had different reasons for their doctors being unavailable. Both ended up serving me the same options over and over again. When I would eventually be referred to transplant, I was met with a cold, bleak man who did not disguise the fact that he didn’t want to work with me. He cared more about the odds than the patient, and he was an asshole. He left a little before I switched healthcare providers.
I was on interferon/ribavirin twice in my life. The odds weren’t in my favor for a repeat prescription. The second time I took it was double the dosage. In hindsight, my specialist knew of several drugs in the phase II and III that I could have waited for, rather than failing a second treatment. The next treatment I was on was an expansion and included Incivek. It would cure my mother, but nearly kill each of us. When the hospital’s preferred insurance at my then-work began to get more expensive I switched to a different insurance and provider.
Upon switching to Sharp, I noticed the difference. The previous healthcare group I’d been with was Scripps, and its surgery and transplant groups are fantastic. Ironically I’d left Scripps when a new transplant doctor started working there. I say this because Sharp handles transplant through Scripps. The new transplant doc was more invested in my well being and very well versed in what was going on in the GI world.
Another delight was my new GI specialist at Sharp. She asked better questions, and within a few meetings she assessed my situation better than any of the GIs I’d had before. I had unknowingly been suffering from ascities for near six years at that point, and it had been becoming more extreme. She was also able to quickly realize that my liver deterioration had led to encephalopathy, something that was evident for near three years by this point. She worked with me and my family to get me on the next two treatments in record time. I took Sovaldi/Olysio as well as Harvoni within weeks of their approval. Her bedside manner, her cooperation with the transplant office, and her willingness to work with my family to make sure these treatments could happen were nothing short of miracles from my experience. She was not hesitant to try new treatments, and she was very well-versed on the new RXs. In combination with the new transplant doc at Scripps, I had an entirely new team of amazing people working on me.
This post however, isn’t about that dramatic shift. It’s about something that I recently found out, regarding my previous GI and his inclination to use Genentech meds over others. I’m an avid fan of the Daily Show, and similarly began following John Oliver’s Last Week Tonight. The show does fantastic bits of journalism with lots of humor built in. Recently they had an episode on prescription drugs that caught my eye. Most of the information wasn’t all that new, however this website was a big deal. It tracks payments regarding doctors and their relationships with pharmaceutical companies.
I looked up my doctors. My new GI was clean, no influence had been bought. My first GI wasn’t on their system, I presume he’s retired to a private practice at this point. My second GI, the doc who’d been so unavailable due to surgeries and speaking/conferences or other out of office things had received over $35,000 in 2013 mostly from Genentech and Boehringer Ingelheim.
Genentech is Pegasys (Interferon) and Ribivirn. The drugs he favored used both of those prescriptions. The trips he took were often at Genentech expense and were labeled as ” Compensation for services other than consulting, including serving as faculty or as a speaker at a venue other than a continuing education program.” Given the information available it can be concluded that he was paid by the company to speak at conferences at their behest. It’s also reasonable to conclude that the over $500 in food/beverage he was given during a collective two and a half weeks were centered around those trips being all inclusive.
BI produces newgen HCV drugs with less than 50% efficacy for Genotype 1a and 1b. He consulted for them and had a number of other sporadic trips and meals. As I know people who still have him as their GI, and we talk about our treatment options and what we learn from docs, I’m certain we’ll see that influence pay into preference for those drugs, given his other records.
Look up your doc, your GI, and see what influence the RX companies are having. And above all, educate yourself on your options.
and for anything else, ask your doctor what your RX options are. If you can wait a day or two ask to make a follow-up (call) to finalize prescribing the right meds, so you can give yourself some time to look up your options. So you can have the best odds.
Information can be your greatest asset in getting the care you need.
As i take my mid-treatment blood draw, i will find out how my viral load is changing. Hopefully this is my fifth and final treatment for Hepatitis C.
I am presently on the Harvoni Treatment from Gilead. I have taken and failed Sovaldi/Olysio, Peg-Interfereon/Ribavirin, and Peg-Interfereon/Ribavirin/Incivek
Since this is a new site, i will be linking both to my personal blog, and my blog on HepMag.
The next few posts will be familiar to those of you know my story. As it’s important to understand how i got to my fifth treatment.
In setting up this new site, I’ve redesigned the symbol for my Liver Life Walk team. The Tilted V, or less than symbol represents my fifth treatment, and that it will be a pivot in my life. It represents how Veritcal Transmission has affected me.
It also represents that the Hep C is less than Me, rather that should say I am greater than HCV.
It also pairs well with HCVME, standing both as the Hepatitis C Virus and me, as well as Hep C is less than me.
As such I feel it wholly represents what i’m attempting to accomplish with this site.
It will serve others: To inform others about the intricacies of navigating life with Hep C, and how impactful small changes and access to information can be.










{kind=link}